| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website https://jocmr.elmerjournals.com |
Original Article
Volume 18, Number 5, May 2026, pages 283-291

Oxidized High-Density Lipoprotein and Cardiovascular Risk in Rheumatoid Arthritis
Linda Scharowa, Susann Patschanb, Nikolaos Pagonasa, Meike Hoffmeisterc, Inga Clausb, Emily Deichslerb, Werner Dammermannd, Oliver Ritterb, Daniel Patschanb, e ![]()
aDepartment of Cardiology und Rhythmology, University Clinic Ruppin-Brandenburg, Brandenburg Medical School (Theodor Fontane), Neuruppin, Brandenburg, Germany
bDepartment of Internal Medicine I - Cardiology, Nephrology and Internal Intensive Medicine, Brandenburg University Hospital, Brandenburg Medical School (Theodor Fontane), Brandenburg an der Havel, Brandenburg, Germany
cInstitute of Biochemistry, Brandenburg Medical School (Theodor Fontane), Brandenburg an der Havel, Brandenburg, Germany
dDepartment of Medicine 2, Gastroenterology, Diabetes, Endocrinology, University Hospital Brandenburg of the Brandenburg Medical School Theodor Fontane, Brandenburg, Germany
eCorresponding Author: Daniel Patschan, University Hospital of Brandenburg, Brandenburg Medical School (Theodor Fontane), Hochstraße 29, 14770 Brandenburg an der Havel, Brandenburg, Germany
Manuscript submitted January 2, 2026, accepted April 7, 2026, published online May 31, 2026
Short title: oxHDL and CVR in RA
doi: https://doi.org/10.14740/jocmr6494
| Abstract | ▴Top |
Background: Patients with rheumatoid arthritis (RA) have a disproportionately increased cardiovascular risk (CVR). Serological CVR predictors that capture this disease-associated risk increase are currently not available. Elevated levels of oxidized high-density lipoprotein (oxHDL) have been associated with coronary artery disease and atrial fibrillation. The aim of this study was to evaluate the suitability of oxHDL as a CVR predictor in RA.
Methods: An observational cross-sectional study was conducted in patients with confirmed RA undergoing variable disease-modifying anti-rheumatic drug (DMARD) therapy. Anamnestic, clinical, and laboratory surrogate markers of cardiovascular morbidity and disease activity were collected. Th quantification of oxHDL was conducted using a fluorometric biochemical cell-free assay.
Results: A total of 200 RA patients were included in the study. oxHDL showed significant correlations with the following variables: body mass index (BMI) (positive), total cholesterol, and average daily prednisolone dose (both negative). Overweight and hypertensive individuals exhibited higher levels of oxHDL. Additionally, oxHDL correlated positively with the number of tender small joints.
Conclusion: oxHDL is associated with distinct CVR indicators in RA. Both prospective and follow-up data are needed to definitively evaluate the role of oxHDL in CVR assessment in RA.
Keywords: oxHDL; RA; Cardiovascular risk; DMARDs; Disease activity
| Introduction | ▴Top |
Patients with rheumatoid arthritis (RA), the most prevalent inflammatory rheumatic disease, are not only at risk due to potentially disabling joint remodeling processes, but also due to a significant increase in the risk of cardiovascular disease and death. This connection can now be considered established, and official recommendations for cardiovascular diagnosis and treatment in RA have already been published [1]. Initially, RA patients accumulate conventional cardiovascular risk (CVR) factors similarly to individuals without systemic autoimmune disorders. However, the disproportionate increase in CVR is primarily attributed to the use of proatherogenic substances, such as glucocorticoids and non-steroidal anti-inflammatory drugs (NSAIDs), as well as the systemic effects of chronic inflammation associated with RA [2]. Consequently, new CVR scores, like QRISK3 [3], include the presence of RA as an independent risk factor. The QRISK3 also proved to be a potent tool for identifying patients with ankylosing spondylitis and increased CVR in recent work [4].
The analysis of lipid status is an essential part of CVR screening. An increase in the high-density lipoprotein fraction (HDL) is known to be associated with CVR reduction. While this association is well-established, the oxidized isoform of HDL (oxHDL) has been discussed to serve as a more precise predictor of cardiovascular events than the total quantity or concentration of HDL [5–7]. The oxidative modification of HDL is triggered by reactive oxygen species and lipid peroxidation radicals, leading to the transformation of HDL into dysfunctional, pro-inflammatory, and pro-atherogenic oxHDL [8, 9]. Unlike native HDL, which promotes reverse cholesterol transport and has anti-inflammatory and antioxidant effects, oxHDL loses these protective functions and becomes pro-inflammatory and pro-atherogenic [10]. Among patients with dyslipidemia, levels of oxHDL have been positively correlated with total HDL cholesterol (HDL-C) [11], suggesting that in certain high-risk contexts a greater total amount of HDL may provide more substrate for oxidative modification. In a 2023 study [12], oxHDL, in contrast to oxidized low-density lipoprotein (oxLDL), was significantly associated with the so-called fibrous burden, i.e. the atherosclerotic plaque burden, over a period of 3.3 years. Therefore, oxHDL may offer certain diagnostic advantages.
The modified form of HDL is subsequently ingested by macrophages, which differentiate into foam cells, a key component of early atherosclerotic plaques [13–15]. To date, increased oxHDL levels were shown in patients with ST-segment elevation myocardial infarction [16], atrial fibrillation (AF) [17], and aortic valve stenosis [18]. In an unpublished in-house study, this parameter has also been identified as a predictor of mortality in patients with newly diagnosed acute kidney injury. To our knowledge, only few investigations on oxHDL in patients with inflammatory rheumatic diseases have been published to date. One study included 33 individuals with RA, seven patients with axial spondyloarthropathy, and four individuals with systemic lupus erythematosus. A higher oxHDL was found in the overall collective examined than in the controls [19]. This study demonstrated that systemic concentrations of oxHDL are altered not only in RA but also in other systemic autoimmune diseases that are etiologically and phenotypically highly heterogeneous. A study published in 2023 also showed lower antioxidant capacity of HDL in RA [20].
The aim of the current study was to analyze oxHDL in only RA. The primary aim was to identify associations between the parameter and CVR surrogate markers. Secondarily, we aimed to investigate possible associations with indicators of disease activity.
| Materials and Methods | ▴Top |
The studied cohort has already been described in a recently published study [21]. Therefore, the clinical characteristics are consistent.
Design
This observational, cross-sectional, single-center study was conducted at the Health Center of Brandenburg University Hospital (Brandenburg Medical School Theodor Fontane) between November 2022 and January 2023. Formal approval was obtained from the Ethics Committee of the Brandenburg Medical School (Neuruppin, Brandenburg, Germany; Approval Number: E-01-20200316). The study adhered to the principles outlined in the Declaration of Helsinki (1975, as revised in 2013). To protect participant confidentiality, all medical and patient data were de-identified, ensuring that individuals could not be identified. The reporting of this study adheres to the STROBE guidelines [22].
Patients
The patients who constituted the subject population of the study were initially identified through screening and subsequently recruited from the Health Center of the Brandenburg University Hospital, which is one of three university hospitals that are affiliated with the Brandenburg Medical School in Germany. Patients who met the following criteria were deemed eligible for inclusion in the study: 1) patients must have been 18 years of age or older at the time of enrollment, and 2) patients must have met the ACR/EULAR 2010 rheumatoid arthritis classification criteria [23]. Furthermore, the therapeutic regimen for the patients included a disease-modifying anti-rheumatic drug (DMARD) therapy, which necessitated the incorporation of either no DMARD (DMARD-native) or a minimum of one conventional or biologic DMARD. The daily dosage of prednisolone was subject to adjustment in accordance with the severity of disease activity. The following criteria were employed for the exclusion of patients from the study: the presence of uncontrolled psychiatric disorders, the existence of additional autoimmune-mediated diseases, the presence of uncontrolled infectious diseases such as human immunodeficiency virus (HIV), hepatitis B or C, and tuberculosis, the presence of uncontrolled drug or alcohol dependence, and the presence of pregnancy.
The patient characteristics that were collected included height, weight, comorbidities, medications, smoking status, and family history of cardiovascular disease. Disease activity was assessed using the Disease Activity Score in 28 joints-C-reactive protein (DAS28-CRP) score, with remission, low, moderate, and high disease activity defined by scores of < 2.6, 2.6 to 3.2, 3.2 to 5.1, and > 5.1, respectively. To assess disease activity, additional tools were employed, including the Visual Analogue Scale (VAS), which ranges from 0 (no pain) to 10 (maximum pain imaginable), a joint assessment for swelling and pain, and the Hannover Functional Questionnaire (HFQ) [24]. The data collected encompassed various aspects related to therapy, including the current DMARD therapy (agent), the use of NSAIDs (dosage and frequency of use), and the daily prednisolone dose in milligrams. Possible correlations or associations with the following indicators of RA disease activity were finally analyzed: VAS, HFQ, DAS28, CRP, and platelet count. Additionally, comparisons were made between individuals who tested positive and negative for rheumatoid factor (RF) and anti-citrullinated protein antibody (ACPA).
The CVR assessment included the following morbidities and laboratory parameters: arterial hypertension, diabetes mellitus including HbA1c (%), past and current smoking (at least 10 cigarettes per day), alcohol consumption (no alcohol, 1–3x per month, 1–3x per week, and daily). Physical activity was categorized as “no physical activity” and “physical activity,” with the following definitions: none, 2–3 times a week, and daily. Total cholesterol (mmol/L), LDL (mmol/L), HDL (mmol/L), and lipoprotein(a) (Lp(a), nmol/L) were also measured. The laboratory parameters measured included RF and ACPA titer, CRP levels (mg/L), complete blood count, and serum creatinine (µmol/L). The following metrics and nominal variables were finally defined and analyzed as CVR factors and morbidities: age, gender, body mass index (BMI), average daily prednisone dosage, serum creatinine, HbA1c, total cholesterol, LDL cholesterol, smoking status, physical exercise, distress, hypertension, known coronary artery disease, known heart failure, family history of atherosclerosis, diabetes mellitus, and obesity.
Quantification of oxHDL
The quantification of oxHDL in serum was conducted using a validated fluorometric biochemical cell-free assay. This assay measures HDL lipid peroxide content based on the oxidation of the fluorochrome Amplex Red. Initially, the serum was depleted of apoB through the process of polyethylene glycol (PEG) precipitation. Subsequently, 50 µL of apoB-depleted serum was added to wells of a 96-well plate in duplicate, followed by the addition of 0.075 units per well of horseradish peroxidase (HRP) and 50 µM Amplex Red reagent, yielding a total volume of 100 µL. HRP has been demonstrated to catalyze the reaction of Amplex Red to resorufin in combination with endogenous peroxides. Following a 1-h incubation period, the fluorescence of resorufin at wavelengths of 535/590 nm was measured using a Spark 10M microplate reader (Tecan). In order to standardize the assay and minimize experimental variability, apoB-depleted sera from 10 healthy volunteers (who were not study participants) were pooled and utilized as experimental control in each plate. The mean fluorescence from each sample was then normalized by the mean fluorescence readout of the pooled control and HDL-C using the following calculation: nHDLox = (HDLox sample × 47 (mg/dL))/(HDLox control × HDL-C sample (mg/dL)), where 47 mg/dL represents the HDL-C of the pooled serum control. The samples were subsequently analyzed following the recruitment of the final patient. The intra-assay coefficient of variation (CV) was 6.7%. The inter-assay coefficient of variation was 3.7%. All laboratory measurements were conducted in the laboratory of the Department of Cardiology und Rhythmology, University Clinic Ruppin-Brandenburg, Brandenburg Medical School (Theodor Fontane), Neuruppin, Brandenburg.
Statistical analysis
Comparisons between nominal data were conducted using the Chi-square test. Metric data were first assessed for normal distribution using the Kolmogorov-Smirnov test. For two-group comparisons, the Mann-Whitney U test was employed, while comparisons among more than two groups were performed using the Kruskal-Wallis test. Correlation analyses between metric data were carried out using Spearman’s correlation analysis. All results were reported as absolute frequencies, percentages, or means ± standard deviation. A P-value of less than 0.05 was considered statistically significant. All statistical analyses were performed using DATAtab software (DATAtab e.U., Graz, Austria).
| Results | ▴Top |
Patients
A total of 200 patients were included in the study (134 women and 66 men). The mean age was 62.5 ± 12.4 years. Of the participants, 127 individuals tested positive for RF, and 109 were positive for ACPA. At the time of study enrollment, the mean DAS28 score was 3.7 ± 1.4. The following DMARD therapies were utilized: methotrexate (MTX) alone 34.5%; MTX in combination 24.5%; DMARD therapy without MTX 14%; early disease prior to DMARD initiation 23.5%; established disease without DMARD therapy 3.5%. Table 1 summarizes all baseline characteristics of the enrolled individuals.
 Click to view | Table 1. Baseline Characteristics of All Included Patients |
oxHDL and CVR
No significant correlations or associations were found with the following variables: age (years) (r = −0.06; P = 0.42), gender (P = 0.30), serum creatinine (µmol/L) (r = 0.11; P = 0.13), HbA1c (%) (r = −0.08; P = 0.29), LDL (mmol/L) (r = 0.04; P = 0.55), smoking status (yes/no) (P = 0.38), physical exercise (yes/no) (P = 0.73), distress (yes/no) (P = 0.21), known coronary artery disease (yes/no) (P = 0.74), known heart failure (yes/no) (P = 0.36), family history of atherosclerosis (yes/no) (P = 0.60), and diabetes mellitus (yes/no) (P = 0.18).
Significant correlations and associations were found with the following variables: BMI (kg/m2) (r = 0.15; P = 0.038), average daily prednisone dosage (mg) (r = −0.25; P = 0.001), total cholesterol (mmol/L) (r = −0.17; P = 0.01), arterial hypertension (yes/no) (P = 0.042), and obesity (yes/no) (P = 0.01). Table 2 provides a comprehensive summary of all results, while Figure 1 illustrates the significant findings.
Click to view | Table 2. Cardiovascular Risk Factor Analysis |
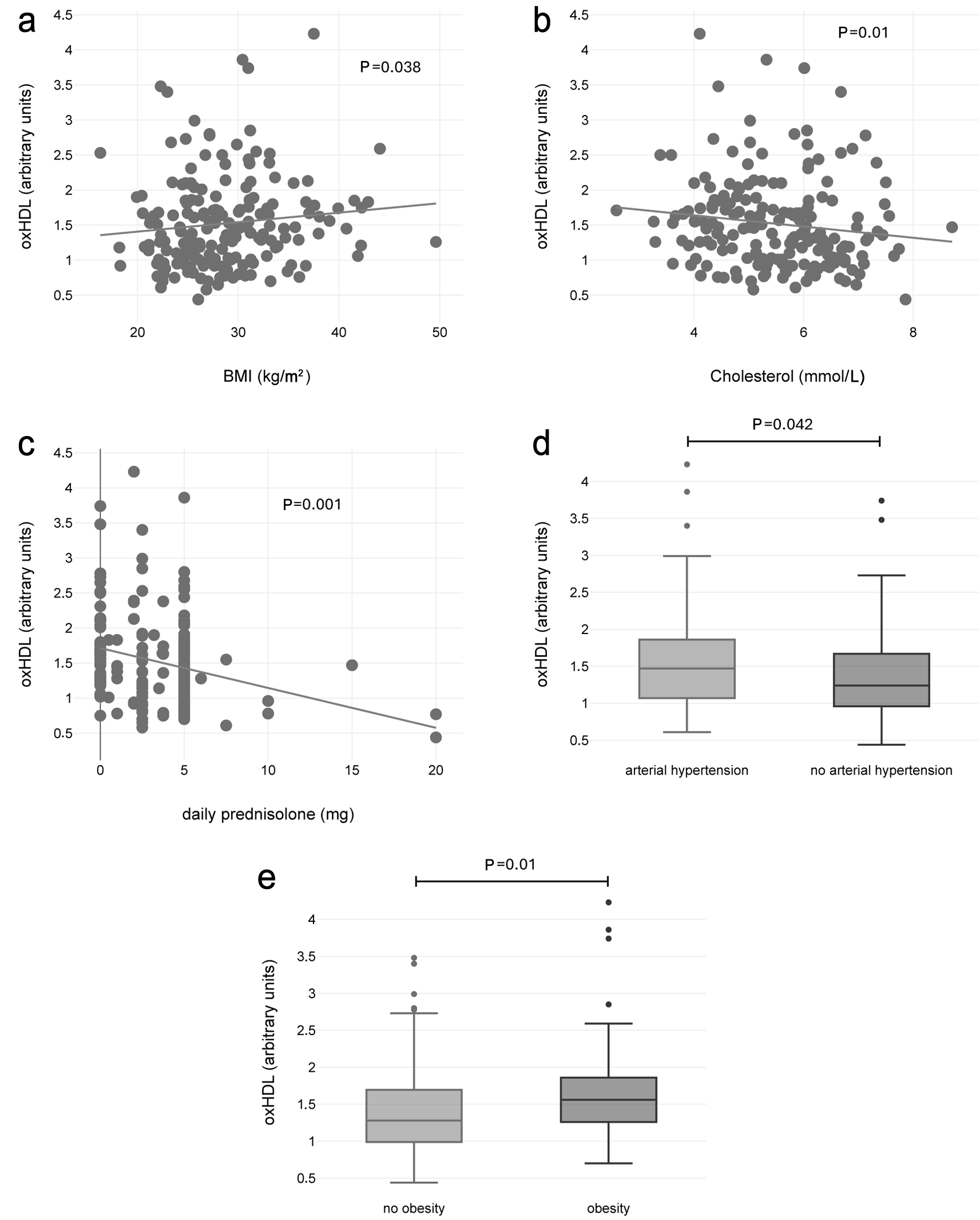 Click for large image | Figure 1. Statistically significant findings from the cardiovascular risk analysis included a positive correlation between oxHDL and BMI (a), as well as negative correlations between oxHDL and total cholesterol (b) and the average daily prednisolone dose (c). Individuals with hypertension (d) and overweight status (e) exhibited higher oxHDL levels. BMI: body mass index; oxHDL: oxidized high-density lipoprotein. |
oxHDL and RA disease activity
No significant correlations or associations were found between oxHDL and the following variables: VAS (r = 0.03; P = 0.6), HFQ (%) (r = 0.05; P = 0.47), DAS28 (r = 0.1; P = 0.19), and CRP (mg/L) (r = −0.12; P = 0.1).
Significant correlations/associations were identified between oxHDL and the platelet count (3 × 105/µL) (r = −0.17; P = 0.021). RF-negative individuals exhibited significantly higher levels of oxHDL (P = 0.018), and the same was true for ACPA-negative patients (P = 0.012). In complementary multiple linear regression analyses, the variables platelet count or RF or ACPA were evaluated with the following covariables: BMI, age, gender. oxHDL has been defined as a dependent variable. The following adjusted P-values were obtained: platelet count 0.43, RF 0.046, and ACPA 0.019. Table 3 and Figure 2 summarize the findings.
Click to view | Table 3. RA Disease Activity Analysis |
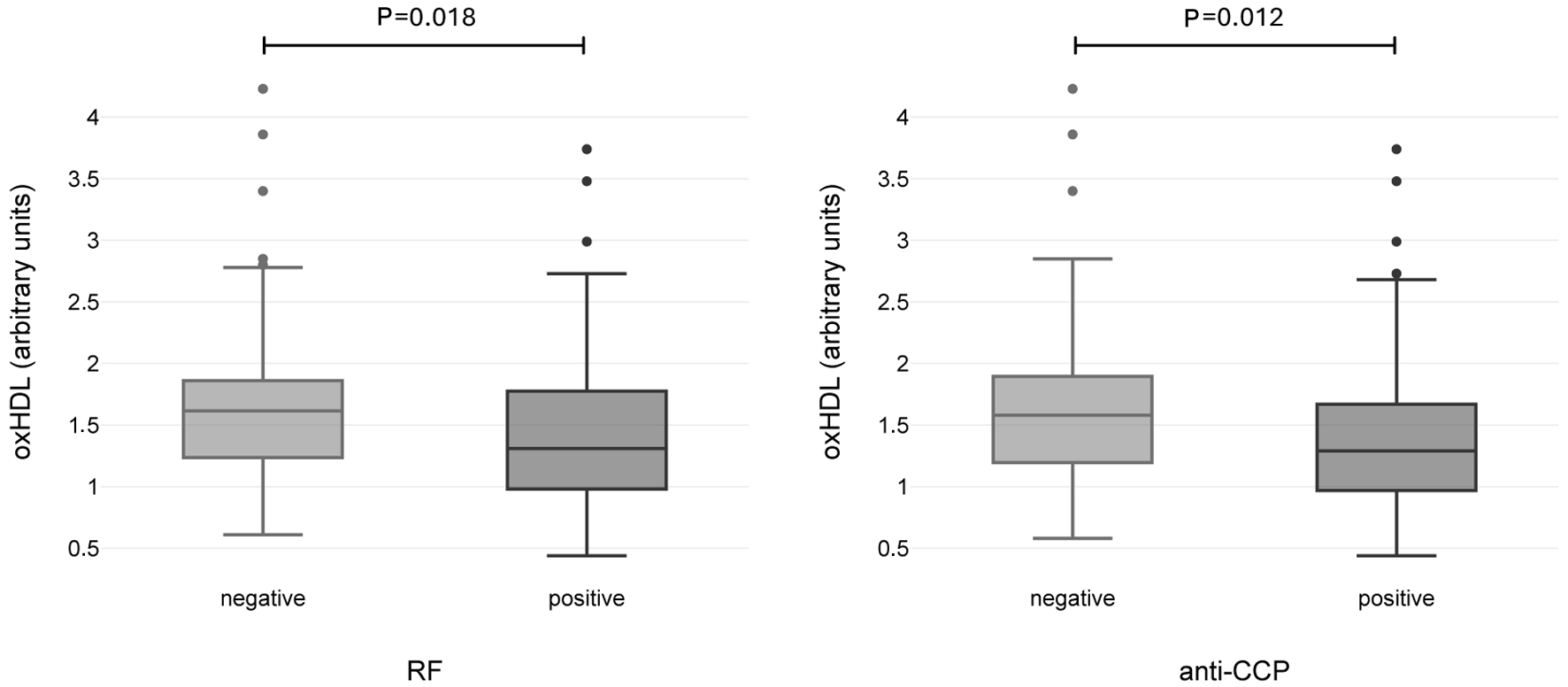 Click for large image | Figure 2. Statistically significant findings from the RA disease activity analysis. Individual with positive RF (a) and positive anti-CCP (b) displayed lower oxHDL, respectively. CCP: cyclic citrullinated peptide; oxHDL: oxidized high-density lipoprotein; RA: rheumatoid arthritis; RF: rheumatoid factor. |
| Discussion | ▴Top |
The primary goal of the investigation was to analyze potential correlations or associations between oxHDL and CVR factors in patients with RA. While relevant findings were undoubtedly identified, the overall pattern of the CVR analysis was inconsistent. Hypertensive and overweight patients exhibited significantly elevated oxHDL levels compared to unaffected individuals, with a positive correlation observed with BMI. Conversely, inverse correlations were found with total cholesterol and the average daily dose of prednisolone. Strictly speaking, an increase in LDL is a well-established CVR factor, yet no positive or negative correlation was observed with this variable. There were no correlations identified with other CVR factors, particularly not with the more potent risk profiles such as diabetes mellitus and chronic kidney disease (as reflected by serum creatinine) [25, 26].
The existing literature presents a rather inconsistent picture regarding the CVR-predictive properties of oxHDL. Nevertheless, there is no doubt that some studies indicated oxHDL as a significant CVR factor. In a prospective investigation involving nearly 900 patients, elevated HDL lipid peroxidation (oxHDL) was associated with confirmed coronary heart disease (CHD). The adjusted odds ratio was 1.69 (95% confidence interval (CI): 1.24–2.38) [27]. In patients undergoing hemodialysis, elevated levels of oxHDL combined with increased interleukin-6 (IL-6) were associated with higher cardiovascular mortality. While oxHDL was not a predictor of overall mortality, it was associated with cardiovascular disease-related events [28]. In a cohort with AF, patients exhibited approximately a 9% higher HDL peroxide level (nHDL_ox). Even after adjustment, this marker remained strongly associated with AF (P ≤ 0.01) [17]. Finally, obese women (BMI > 30) exhibited elevated oxHDL levels, along with inflammatory markers, even in the absence of manifest CHD [17]. However, conflicting findings have also been published. Prospectively, lower oxHDL levels were associated with reduced progression of coronary calcification (Agatston score) [29]. In a cohort of CAD patients, oxHDL demonstrated an inverse association with high-risk plaque features, such as necrotic and fibro-fatty burden. Lower oxHDL levels were linked to unfavorable plaque characteristics. Notably, oxHDL proved to be a better predictor than HDL-C or oxLDL [12]. An explanation for these conflicting results can partially be provided by considering some of the following features: there is no standardized method for measuring oxHDL, as different studies employ various detection techniques (e.g., enzyme-linked immunosorbent assay (ELISA), mass spectrometry) that identify distinct modifications of HDL (such as oxidized ApoA-I, lipid peroxidation of HDL particles, etc.) [30]. Some tests detect mild oxHDL, which may still retain its functionality, while others target heavily modified HDL that has lost its protective properties. OxHDL may still be functional in certain contexts (for example, cholesterol uptake), but when extensively modified, it can exert pro-inflammatory effects [31]. In early stages of atherosclerosis, mild HDL oxidation can serve as an adaptive mechanism, exerting antioxidant or anti-inflammatory effects. However, in later stages or under conditions of chronic oxidative stress, oxHDL can become dysfunctional, developing pro-inflammatory or pro-atherogenic characteristics. However, the final aspect appears to have only some validity, as illustrated by the previously cited study by Sorokin et al [12].
The interpretation of our data is further complicated by the fact that the survey was conducted at a single point in time. Additionally, our study lacks a non-rheumatic control group with comparable characteristics such as age, gender, and other relevant factors. Currently, regarding CVR prediction in RA, it can only be concluded that oxHDL may potentially be helpful under certain conditions in assessing atherosclerosis susceptibility; however, a general suitability as a new CVR factor in RA cannot be established at this time. A final aspect to note concerns the possible effects of glucocorticoids on HDL/oxHDL metabolism. As early as 2020 [32], it was proven that systemic glucocorticoids can result in increased production of dysfunctional HDL. The steroids regularly used in our collective will have potentially had an influence on the results, even if the exact effect is difficult to estimate at the moment.
Regarding the suitability of oxHDL as an additional activity parameter for RA, differences in lipid concentrations were exclusively identified between seropositive and seronegative individuals. No associations were found with established activity indices such as CRP and DAS28. Therefore, it currently cannot be reliably concluded that oxHDL is a dependable candidate for assessing disease activity in RA.
Limitations
First, the number of participants in the study is limited. It is a cross-sectional snapshot, and therefore, we cannot draw conclusions about cardiovascular morbidity or mortality based on our data. Another limitation is the absence of a non-RA comparison group with similar epidemiological and clinical characteristics.
Conclusions
OxHDL was associated with several indicators of cardiovascular morbidity. Because the study had a retrospective design, only very limited conclusions can be drawn. The collected data do not support oxHDL as a possible candidate for CVR assessment in RA, both prospective and follow-up data are needed to definitively answer this question.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
The authors declare that they have no conflict of interest.
Informed Consent
All participants gave their written informed consent prior to enrolment.
Author Contributions
Linda Scharow performed the oxHDL quantification and analysis of the results. Susann Patschan designed the study and recruited all patients. Nikolaos Pagonas assisted in oxHDL quantification. Meike Hoffmeister analyzed data. Inga Claus helped in patient recruitment. Emily Deichsler recruited patients. Werner Dammermann assisted in oxHDL quantification. Oliver Ritter prepared figures and tables. Daniel Patschan wrote the article. All authors approved the final version of the article.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Agca R, Heslinga SC, Rollefstad S, Heslinga M, McInnes IB, Peters MJ, Kvien TK, et al. EULAR recommendations for cardiovascular disease risk management in patients with rheumatoid arthritis and other forms of inflammatory joint disorders: 2015/2016 update. Ann Rheum Dis. 2017;76(1):17-28.
doi pubmed - Choy E, Ganeshalingam K, Semb AG, Szekanecz Z, Nurmohamed M. Cardiovascular risk in rheumatoid arthritis: recent advances in the understanding of the pivotal role of inflammation, risk predictors and the impact of treatment. Rheumatology (Oxford). 2014;53(12):2143-2154.
doi pubmed - Kim SH, Lee SH, Kim HR, Min HK. Cardiovascular disease risk calculators to reflect the subclinical atherosclerosis of coronary artery in rheumatoid arthritis: a pilot study. BMC Rheumatol. 2021;5(1):39.
doi pubmed - Polo YlBJ, Castaneda S, Sanchez-Alonso F, Plaza Z, Garcia-Gomez C, Ferraz-Amaro I, Erausquin C, et al. Combined use of QRISK3 and SCORE2 increases identification of ankylosing spondylitis patients at high cardiovascular risk: Results from the CARMA Project cohort after 7.5 years of follow-up. Semin Arthritis Rheum. 2024;66:152442.
doi pubmed - Navab M, Reddy ST, Van Lenten BJ, Fogelman AM. HDL and cardiovascular disease: atherogenic and atheroprotective mechanisms. Nat Rev Cardiol. 2011;8(4):222-232.
doi pubmed - Linton MF, Yancey PG, Tao H, Davies SS. HDL function and atherosclerosis: reactive dicarbonyls as promising targets of therapy. Circ Res. 2023;132(11):1521-1545.
doi pubmed - Khera AV, Cuchel M, de la Llera-Moya M, Rodrigues A, Burke MF, Jafri K, French BC, et al. Cholesterol efflux capacity, high-density lipoprotein function, and atherosclerosis. N Engl J Med. 2011;364(2):127-135.
doi pubmed - Trakaki A, Marsche G. Current Understanding of the immunomodulatory activities of high-density lipoproteins. Biomedicines. 2021;9(6):587.
doi pubmed - Undurti A, Huang Y, Lupica JA, Smith JD, DiDonato JA, Hazen SL. Modification of high density lipoprotein by myeloperoxidase generates a pro-inflammatory particle. J Biol Chem. 2009;284(45):30825-30835.
doi pubmed - Ouyang FW, Chiang HH, Hsu WL, Tsai MH, Huang CY, Remaley AT, Akyol O, et al. Dysfunctional high-density lipoprotein: an updated review. Front Cardiovasc Med. 2025;12:1713387.
doi pubmed - Kotani K, Sakane N, Ueda M, Mashiba S, Hayase Y, Tsuzaki K, Yamada T, et al. Oxidized high-density lipoprotein is associated with increased plasma glucose in non-diabetic dyslipidemic subjects. Clin Chim Acta. 2012;414:125-129.
doi pubmed - Sorokin AV, Hong CG, Aponte AM, Florida EM, Tang J, Patel N, Baranova IN, et al. Association of oxidized ApoB and oxidized ApoA-I with high-risk coronary plaque features in cardiovascular disease. JCI Insight. 2023;8(20):e172893.
doi pubmed - Sini S, Deepa D, Harikrishnan S, Jayakumari N. High-density lipoprotein from subjects with coronary artery disease promotes macrophage foam cell formation: role of scavenger receptor CD36 and ERK/MAPK signaling. Mol Cell Biochem. 2017;427(1-2):23-34.
doi pubmed - Holzer M, Gauster M, Pfeifer T, Wadsack C, Fauler G, Stiegler P, Koefeler H, et al. Protein carbamylation renders high-density lipoprotein dysfunctional. Antioxid Redox Signal. 2011;14(12):2337-2346.
doi pubmed - Marsche G, Hammer A, Oskolkova O, Kozarsky KF, Sattler W, Malle E. Hypochlorite-modified high density lipoprotein, a high affinity ligand to scavenger receptor class B, type I, impairs high density lipoprotein-dependent selective lipid uptake and reverse cholesterol transport. J Biol Chem. 2002;277(35):32172-32179.
doi pubmed - Li BQ, Zhong YC, Wang X. Plasma oxidized high-density lipoprotein and glycated apolipoprotein A-I concentrations in ST-segment elevation myocardial infarction patients with stress hyperglycaemia or high thrombus burden. Ups J Med Sci. 2018;123(3):158-166.
doi pubmed - Pagonas N, Mueller R, Weiland L, Jaensch M, Dammermann W, Seibert FS, Hillmeister P, et al. Oxidized high-density lipoprotein associates with atrial fibrillation. Heart Rhythm. 2024;21(4):362-369.
doi pubmed - Sun JT, Chen YY, Mao JY, Wang YP, Chen YF, Hu X, Yang K, et al. Oxidized HDL, as a novel biomarker for calcific aortic valve disease, promotes the calcification of aortic valve interstitial cells. J Cardiovasc Transl Res. 2019;12(6):560-568.
doi pubmed - Waldecker-Gall S, Seibert F, Bertram S, Doevelaar A, Braun J, Baraliakos X, Babel N, et al. Dysfunctional high-density lipoprotein in chronic inflammatory rheumatic diseases. Ther Adv Musculoskelet Dis. 2023;15:1759720X231187191.
doi pubmed - Garcia-Gomez MC, Padro T, Munoz-Garcia N, Bianchi M, Alvarez L, Badimon L, Corbella E, et al. Dysfunctional antioxidant capacity of high-density lipoprotein in rheumatoid arthritis. Eur J Clin Invest. 2023;53(8):e13999.
doi pubmed - Claus I, Hoffmeister M, Strathmeyer S, Heelemann S, Remus C, Dammermann W, Ritter O, et al. Metabolomics for distinguishing cardiovascular risk in rheumatoid arthritis across different disease-modifying antirheumatic drug therapies. J Clin Med Res. 2025;17(2):89-96.
doi pubmed - von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, Initiative S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):e296.
doi pubmed - Kay J, Upchurch KS. ACR/EULAR 2010 rheumatoid arthritis classification criteria. Rheumatology (Oxford). 2012;51(Suppl 6):vi5-9.
doi pubmed - Lautenschlager J, Mau W, Kohlmann T, Raspe HH, Struve F, Bruckle W, Zeidler H. [Comparative evaluation of a German version of the Health Assessment Questionnaire and the Hannover Functional Capacity Questionnaire]. Z Rheumatol. 1997;56(3):144-155.
doi pubmed - Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296-1305.
doi pubmed - Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2024;105(4S):S117-S314.
doi pubmed - Pagonas N, Mueller R, Weiland L, Jaensch M, Westhoff TH, Buschmann IR, et al. Oxidation of HDL in patients with coronary artery disease. Eur Heart J. 2020;41(Supplement_2):ehaa946.1521.
doi - Honda H, Ueda M, Kojima S, Mashiba S, Michihata T, Takahashi K, Shishido K, et al. Oxidized high-density lipoprotein as a risk factor for cardiovascular events in prevalent hemodialysis patients. Atherosclerosis. 2012;220(2):493-501.
doi pubmed - Miki T, Miyoshi T, Kotani K, Kohno K, Asonuma H, Sakuragi S, Koyama Y, et al. Decrease in oxidized high-density lipoprotein is associated with slowed progression of coronary artery calcification: Subanalysis of a prospective multicenter study. Atherosclerosis. 2019;283:1-6.
doi pubmed - Matsunaga T, Koyama I, Hokari S, Komoda T. Detection of oxidized high-density lipoprotein. J Chromatogr B Analyt Technol Biomed Life Sci. 2002;781(1-2):331-343.
doi pubmed - Wang Y, Ji L, Jiang R, Zheng L, Liu D. Oxidized high-density lipoprotein induces the proliferation and migration of vascular smooth muscle cells by promoting the production of ROS. J Atheroscler Thromb. 2014;21(3):204-216.
doi pubmed - Bouillet B, Gautier T, Denimal D, Samson M, Masson D, Pais de Barros JP, Maquart G, et al. Glucocorticoids impair HDL-mediated cholesterol efflux besides increased HDL cholesterol concentration: a proof of concept. Eur J Endocrinol. 2020;183(3):297-306.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Clinical Medicine Research is published by Elmer Press Inc.