Figures
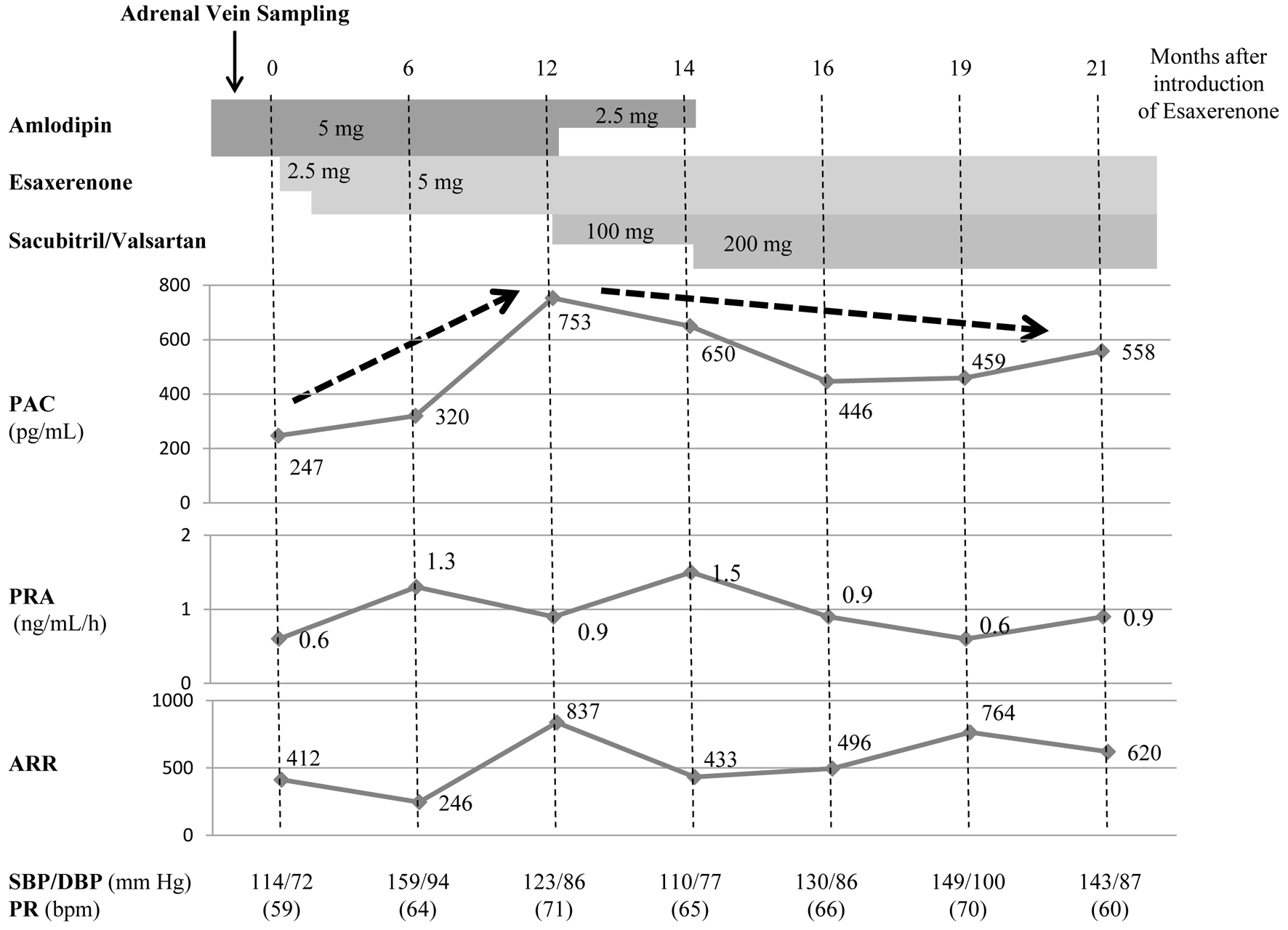
↓ Figure 1. Case 1 involved a patient with
primary aldosteronism likely caused by an aldosterone-producing adenoma (calcium channel blocker
→ sacubitril/valsartan). The patient was on amlodipine, with insufficient reduction in BP.
Therefore, esaxerenone was added, although BP still did not decrease sufficiently, and the PAC
increased. Amlodipine was subsequently changed to sacubitril/valsartan; PRA temporarily increased, and
the PAC gradually decreased. PAC: plasma aldosterone concentration; PRA: plasma renin activity; ARR:
aldosterone-to-renin ratio; SBP: systolic blood pressure; DBP: diastolic blood pressure; PR: pulse rate;
bpm: beats per minute.
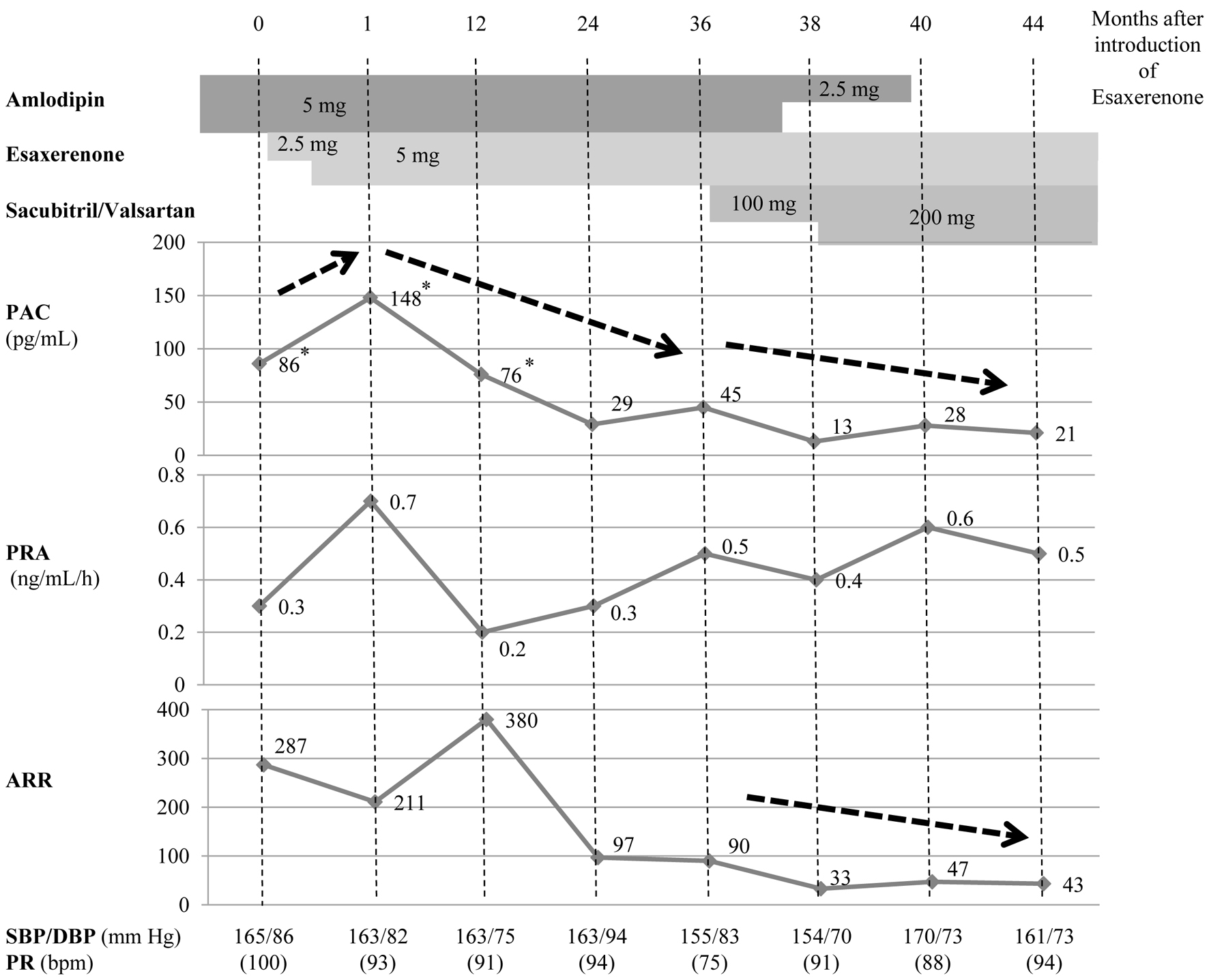
↓ Figure 2. Case 2 involved a patient with
primary aldosteronism likely caused by idiopathic hyperaldosteronism (calcium channel blocker →
sacubitril/valsartan). Although the addition of esaxerenone led to an increased PAC, PRA did not
sufficiently increase. About 3 years after esaxerenone was added, the PAC gradually decreased. After
switching amlodipine to sacubitril/valsartan, the PAC and ARR decreased slightly. *PAC values measured
by radioimmunoassay prior to March 2021 have been converted to values consistent with the use of CLEIA
to reflect changes in the standard assay used to measure PAC [19]. PAC: plasma aldosterone
concentration; PRA: plasma renin activity; ARR: aldosterone-to-renin ratio; CLEIA: chemiluminescent
enzyme immunoassay.
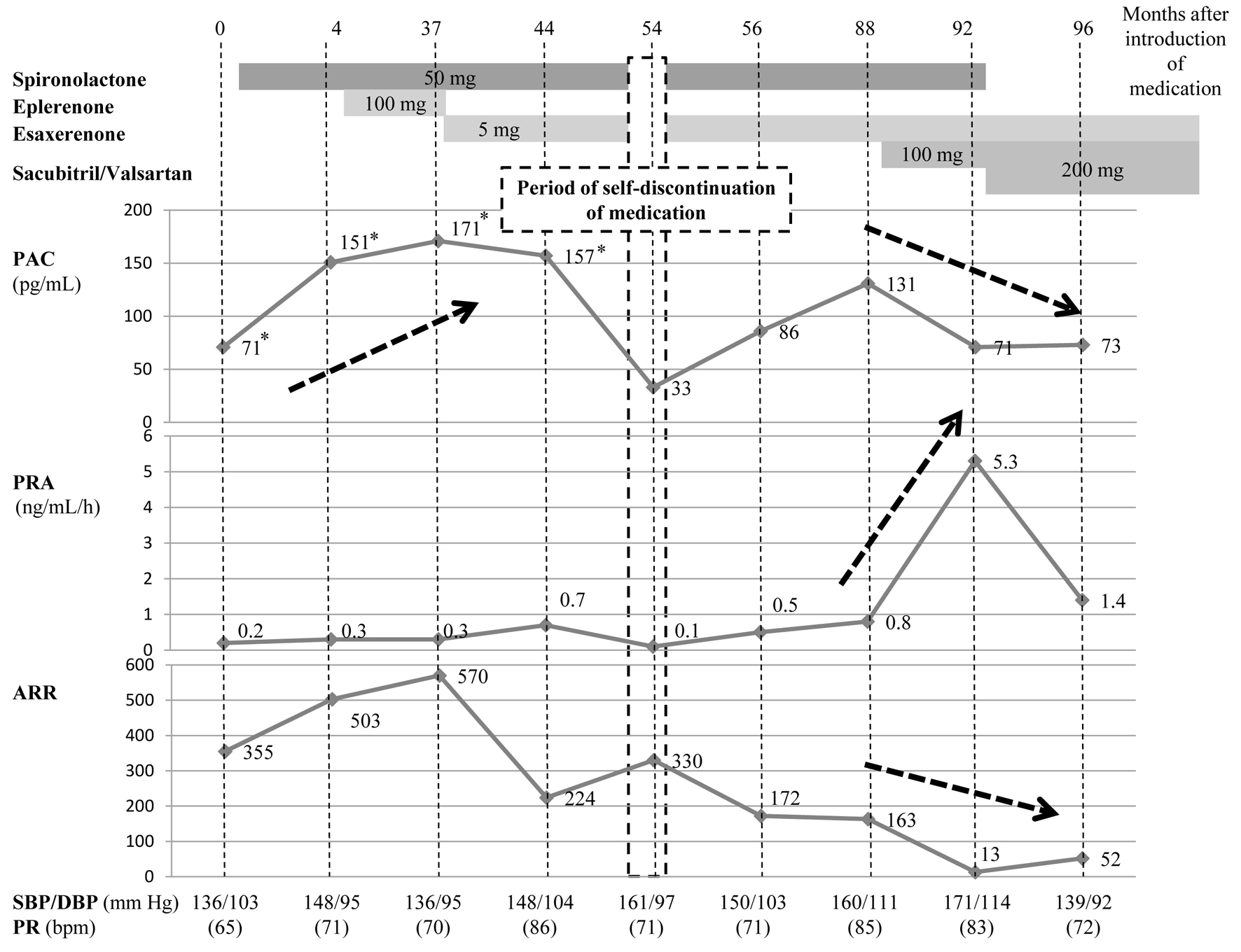
↓ Figure 3. Case 3 involved a patient with
primary aldosteronism likely caused by idiopathic hyperaldosteronism (spironolactone →
sacubitril/valsartan). Although eplerenone was changed to esaxerenone, PRA did not exceed 1.0 ng/mL/h.
After the patient temporarily self-discontinued treatment, the PAC (which had been elevated with
mineralocorticoid receptor antagonist decreased, and PRA was again suppressed as a result of primary
aldosteronism. After the medication regimen was resumed, sacubitril/valsartan was added. Because PRA
markedly increased and the PAC decreased, spironolactone was discontinued, and sacubitril/valsartan was
increased to the maximum dose. Finally, the PAC and ARR decreased, and PRA remained above 1.0 ng/mL/h.
PAC: plasma aldosterone concentration; PRA: plasma renin activity; ARR: aldosterone-to-renin ratio.
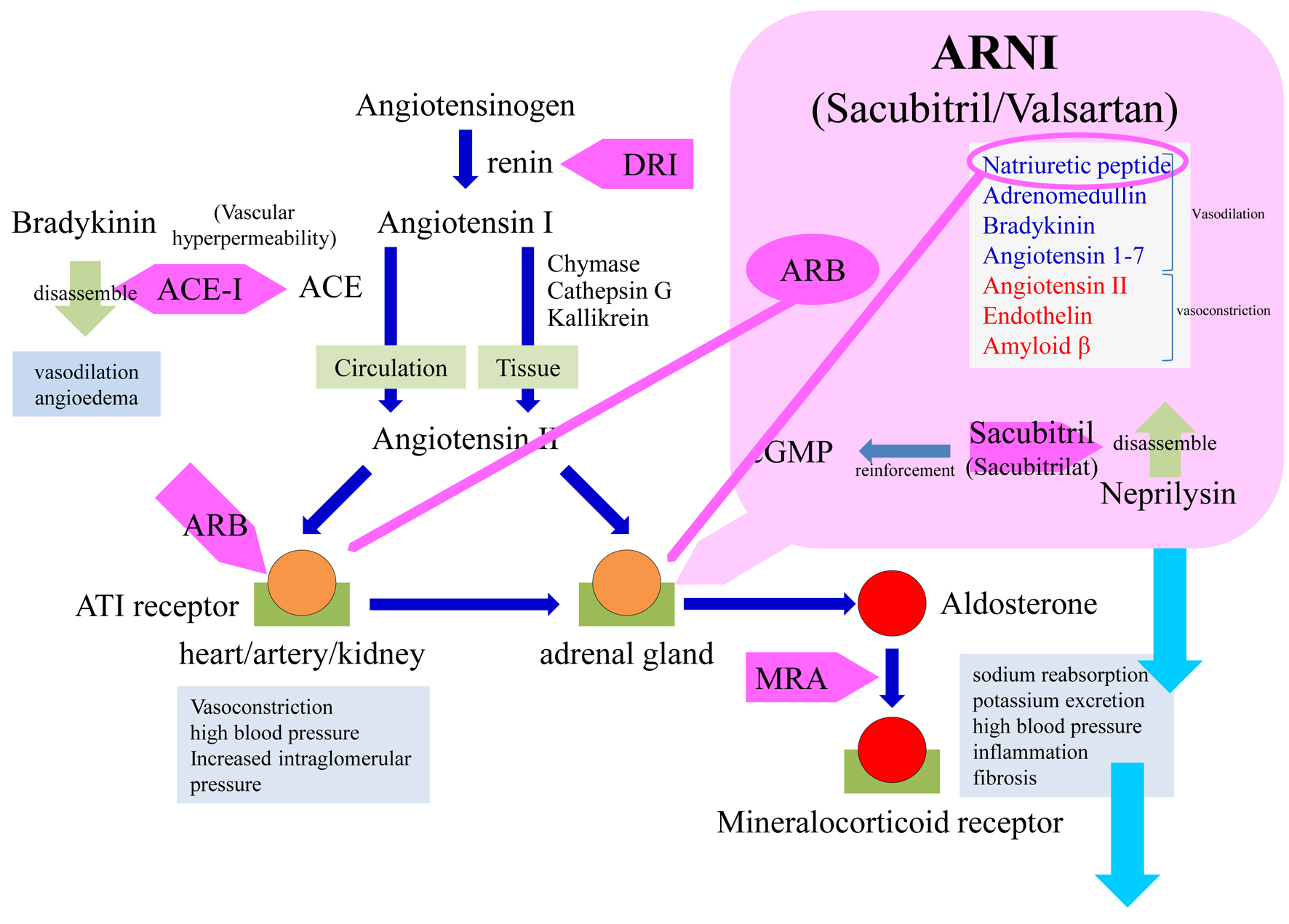
↓ Figure 4. Schema of the
renin-angiotensin-aldosterone system and sacubitril/valsartan. As valsartan blocks angiotensin II type 1
receptors and sacubitril exerts a natriuretic peptide-mediated effect on the adrenal glands, the
combination of sacubitril/valsartan directly suppresses aldosterone production and secondarily
suppresses the mineralocorticoid receptor-mediated effect. Because the mineralocorticoid receptor is
blocked by administration of an MRA, however, positive feedback activates the RAAS and stimulates
aldosterone production. ACE: angiotensin-converting enzyme; ACE-I: angiotensin-converting enzyme
inhibitor; ARB: angiotensin receptor blocker; ARNI: angiotensin receptor-neprilysin inhibitor; AT:
angiotensin; cGMP: cyclic guanosine monophosphate; DRI: direct renin inhibitor; MRA: mineralocorticoid
receptor antagonist; RAAS: renin-angiotensin-aldosterone system.