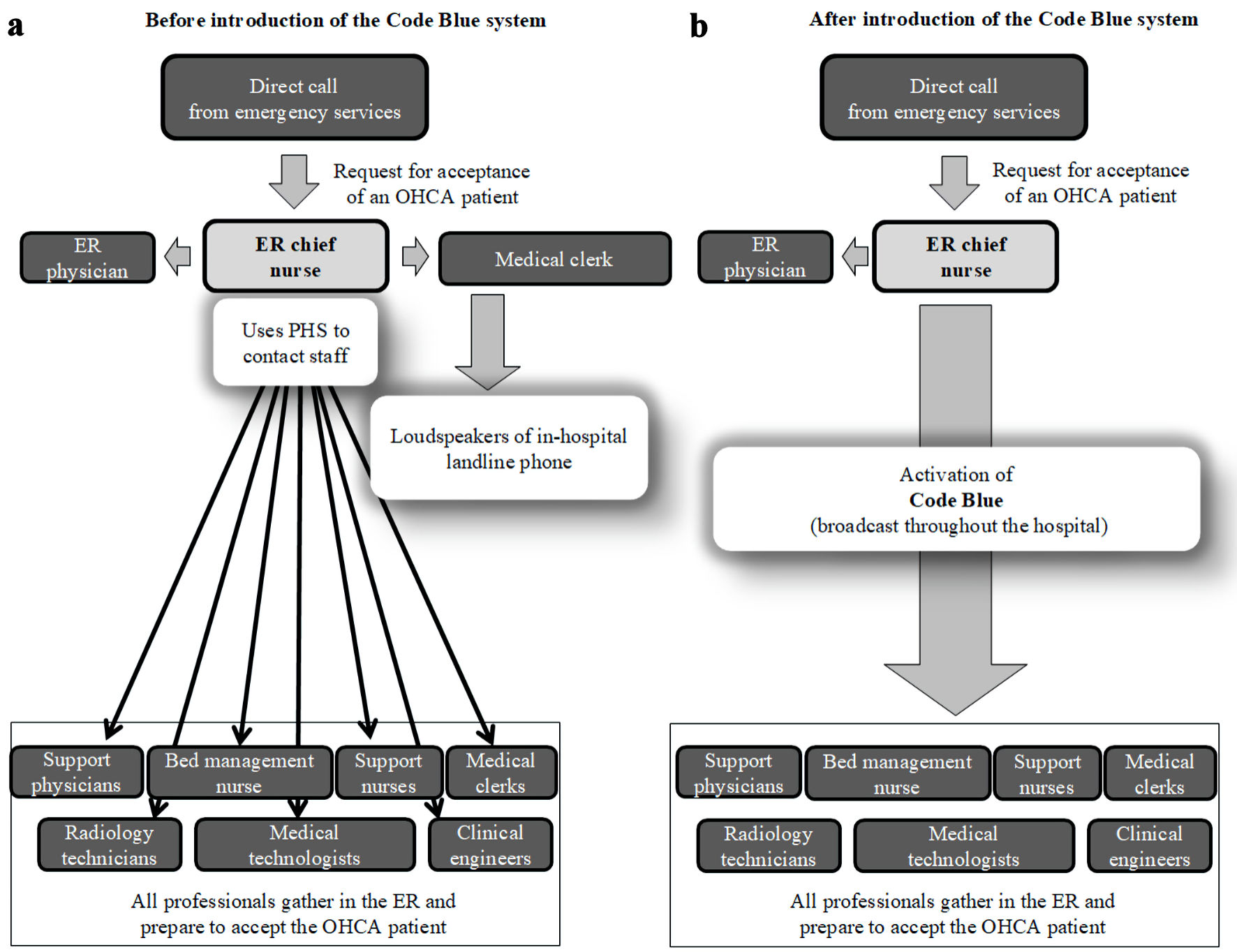
↓ Figure 1. Comparison of communication systems
used to gather staff in the ER in preparation for accepting OHCA patients. (a) Situation before
introduction of the Code Blue system. (b) After the introduction of the Code Blue system. For example,
if a patient with OHCA will arrive in 10 min, the ER nurse will twice broadcast “Code Blue, Code
Blue, 10 minutes” via the Code Blue system. ER: emergency room; OHCA: out-of-hospital cardiac
arrest; PHS: personal handy phone system.