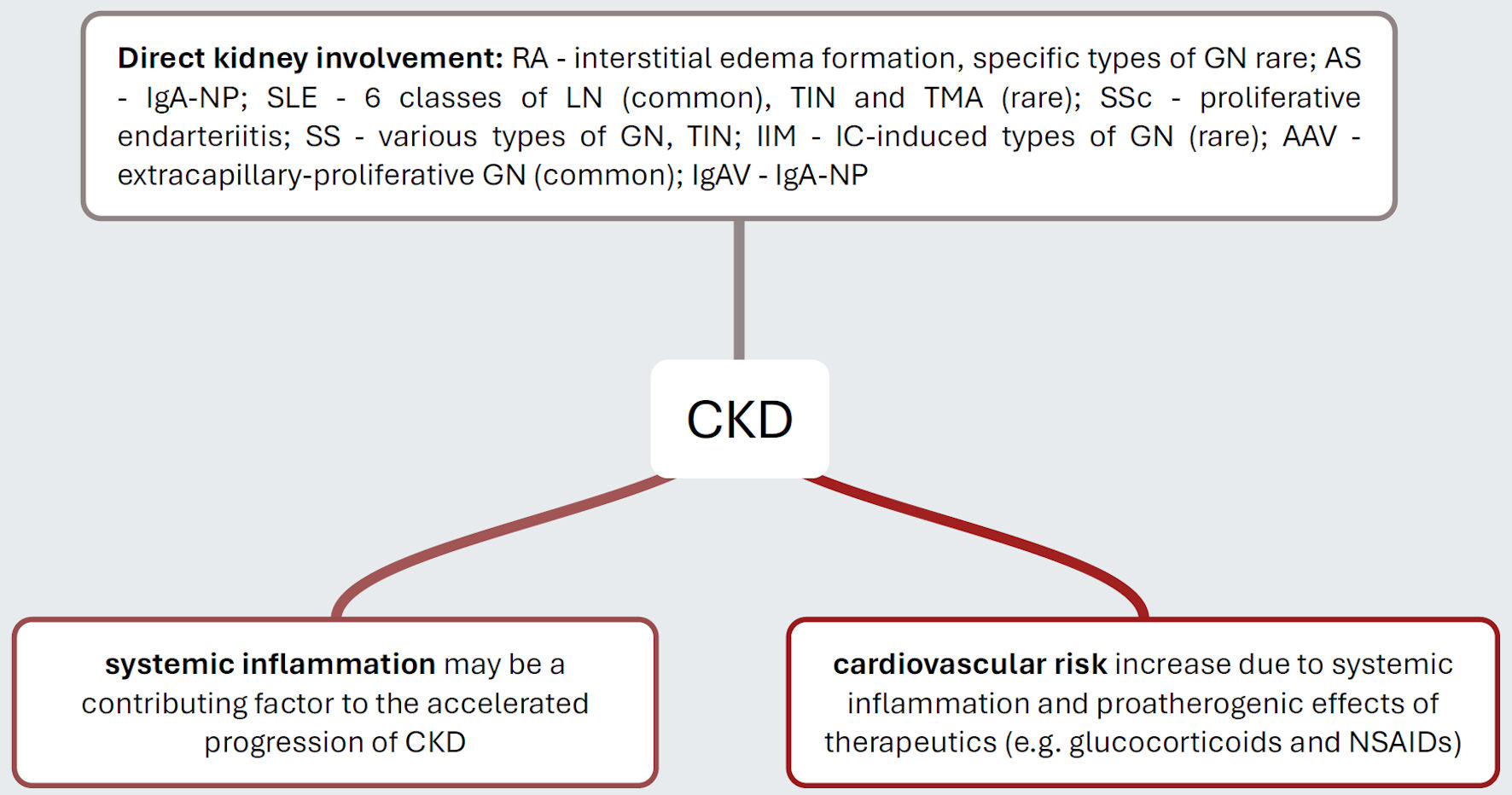
↓ Figure 1. Pathogenetic mechanisms that explain
the increased risk of CKD in distinct inflammatory rheumatic diseases. Rheumatic autoimmunopathies
manifest themselves with varying frequency directly on the kidneys, with SLE and AAV being
disproportionately common. It is now considered certain that individuals with rheumatic
autoimmunopathies suffer from a significantly increased cardiovascular risk, which ultimately increases
the risk of hypertensive atherosclerotic nephropathy. Presumably, the inflammatory activity of the
diseases themselves is also a progression-promoting factor. CKD: chronic kidney disease; RA: rheumatoid
arthritis; GN: glomerulonephritis; IgA-NP: IgA nephropathy; SLE: systemic lupus erythematosus; LN: lupus
nephritis; TIN: tubulo-interstitial nephritis; TMA: thrombotic microangiopathy; SSc: systemic sclerosis;
SS: Sjogren’s syndrome; IIM: idiopathic inflammatory myopathy; IC: immunocomplex; AAV:
ANCA-associated vasculitis; IgAV: IgA vasculitis; NSAIDs: nonsteroidal anti-inflammatory drugs.