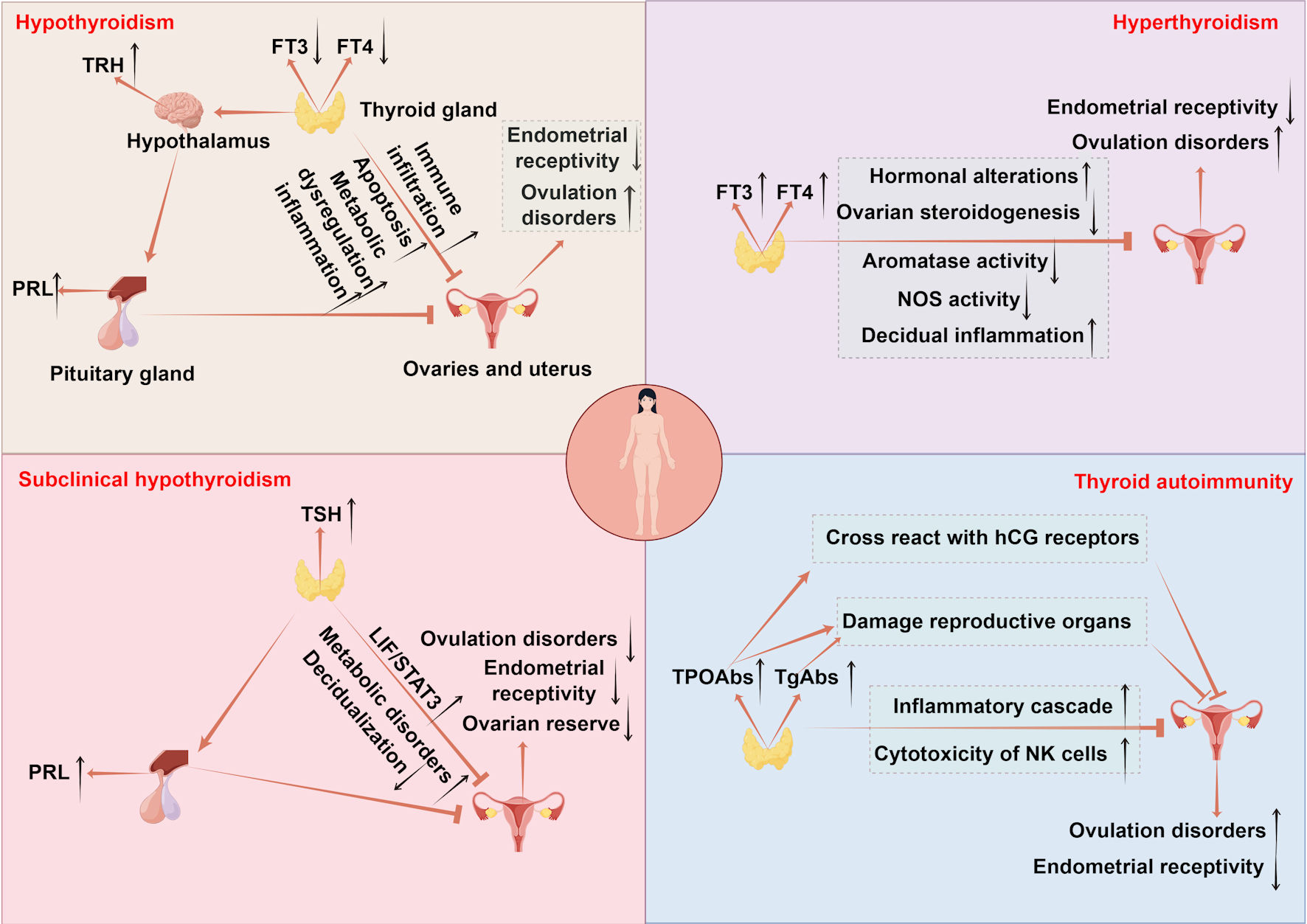
↓ Figure 1. The mechanisms of thyroid disorders
affecting female fertility. Hypothyroidism disrupts follicular development via CHOP and
caspase3-mediated apoptosis and causes metabolic imbalance in lipids and glucose accompanied by immune
infiltration, impairing ovarian and uterine function. Endometrial receptivity is diminished due to low
E2 osteopontin and HOXA10, while uterine gland function is impaired with reduced integrins and LIF and
increased MUC1. Uterine hyperplasia and inflammation occur due to elevated VEGF-A, alongside decreased
PLINA, TAG and TC. Hyperprolactinemia from excessive TRH and menstrual irregularities further reduce
fertility. Hyperthyroidism leads to infertility by elevating SHBG and estradiol which disrupts
folliculogenesis through impaired antral follicle growth and dysregulated NOS expression. It also
suppresses FSH stimulated aromatase activity in ovarian steroidogenesis and causes decidual imbalance
with elevated DBA-positive uNK cells and abnormal cytokine production. SCH contributes to infertility by
promoting metabolic dysregulation in lipids and glucose and hyperprolactinemia reducing ovarian reserve
and upregulating LIF/STAT3 signaling, which collectively impair endometrial receptivity and
decidualization. TAI drives follicular inflammation through IFNγ-induced CXCL9/10/11-mediated
recruitment of CXCR3+ T cells and enhances NK cell cytotoxicity. Non organ specific
antibodies cross react with trophoblasts and disrupt Th1/Th2 balance promoting implantation failure and
pregnancy loss. TPOAbs cross reactivity with hCG receptors on the zona pellucida, direct damage by TPOAb
and TgAb to reproductive tissues, and reduced ovarian reserve and embryo quality further contribute to
reproductive impairment. TSH: thyroid-stimulating hormone; FT4: free thyroxine; FT3: free
triiodothyronine; CHOP: C/EBP homologous protein; TAG: triacylglycerol; HOXA10: homeobox A10; LIF:
leukemia inhibitory factor; MUC1: mucin 1; VEGF-A: vascular endothelial growth factor A; PLIN-A:
perilipin A; DBA: dolichos biflorus agglutinin; uNK: uterine natural killer; IFNγ:
interferon-γ; CXCL9/10/11: CXC chemokine ligands 9; CXCR3: CXC chemokine receptor 3; TRH:
thyrotropin-releasing hormone; FSH: follicle-stimulating hormone; SHBG: sex hormone-binding globulin;
NOS: nitric oxide synthase; PRL: prolactin; TPOAbs: thyroid peroxidase antibodies; TgAbs: thyroglobulin
antibodies; hCG: human chorionic gonadotropin; SCH: subclinical hypothyroidism; TAI: thyroid
autoimmunity.