Figures
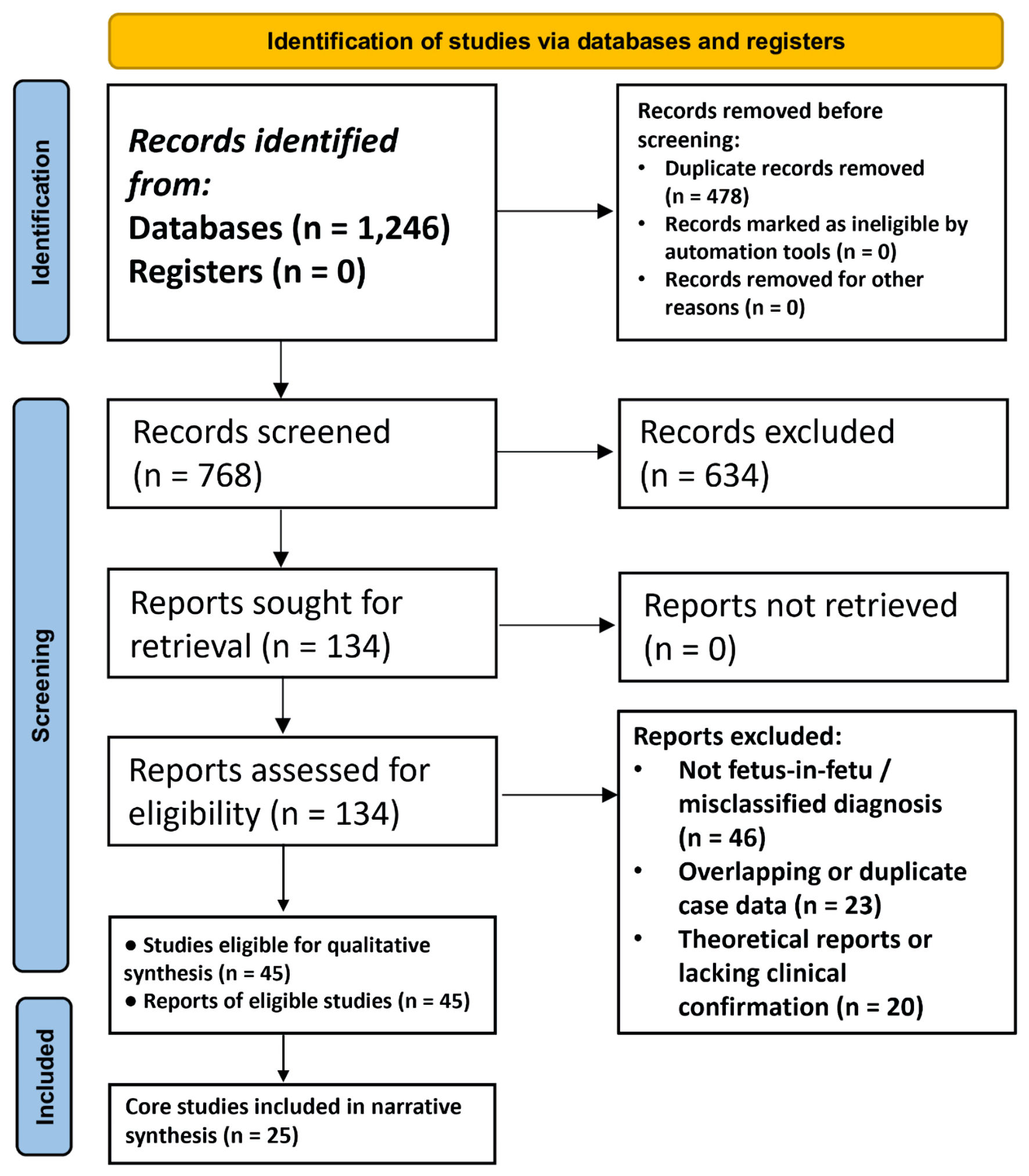
↓ Figure 1. PRISMA 2020 flow diagram of study identification, screening, eligibility, and inclusion. This PRISMA 2020 flow diagram summarizes the identification and selection of studies evaluating fetus-in-fetu (FIF). A total of 1,246 records were identified through database searching (PubMed, EMBASE, Scopus, and Google Scholar). After removal of duplicate records, 768 unique records underwent title and abstract screening, of which 634 were excluded for irrelevance or misclassification. Full-text assessment was performed for 134 reports, with 89 excluded due to absence of confirmed FIF diagnosis, overlapping or duplicate case data, or insufficient clinical confirmation. In total, 45 studies met eligibility criteria for qualitative synthesis. From these, a core subset of 25 studies was selected for focused narrative synthesis and detailed citation in this review, based on predefined criteria emphasizing diagnostic certainty, clinical relevance, methodological completeness, and avoidance of overlapping case reporting. This two-stage inclusion approach aligns with PRISMA principles while allowing transparent and focused synthesis in the context of a rare condition with heterogeneous reporting. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
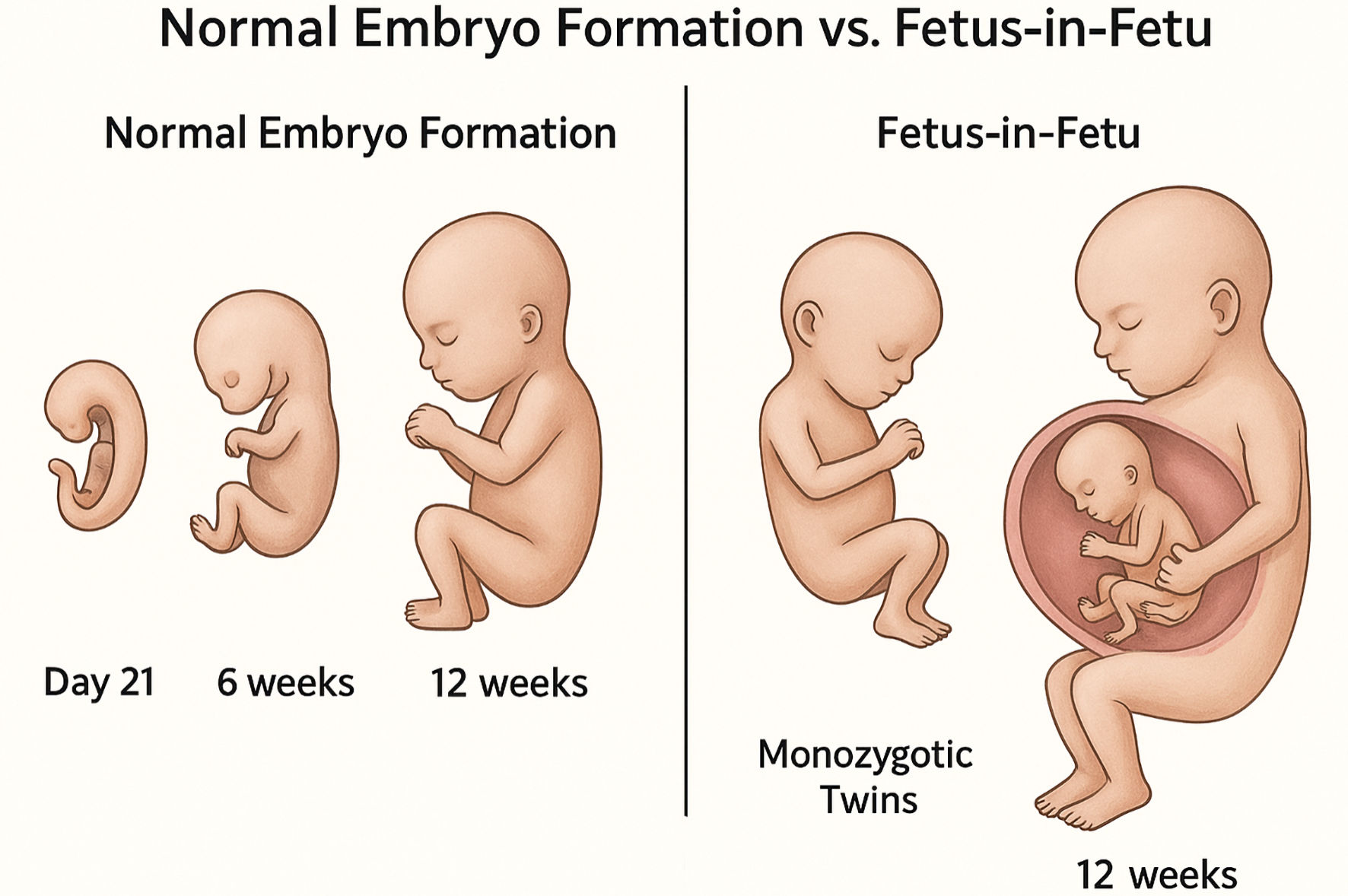
↓ Figure 2. Schematic comparison of normal embryonic development and fetus-in-fetu (FIF) formation. This schematic illustrates key developmental differences between normal human embryogenesis and the proposed mechanism underlying FIF formation. In normal development, the zygote undergoes sequential cleavage, implantation, and organogenesis, resulting in a single, normally formed fetus. In the FIF pathway, incomplete separation of monozygotic twins during early post-implantation development leads to incorporation of one twin within the body of the host. The parasitic twin demonstrates arrested growth, remains dependent on the host’s circulation, and may develop rudimentary axial and limb structures. This figure is a conceptual representation synthesized from established embryological principles and clinical observations reported in the literature and is not derived from a single experimental or imaging dataset. Relative size and developmental timing are illustrative rather than to scale.
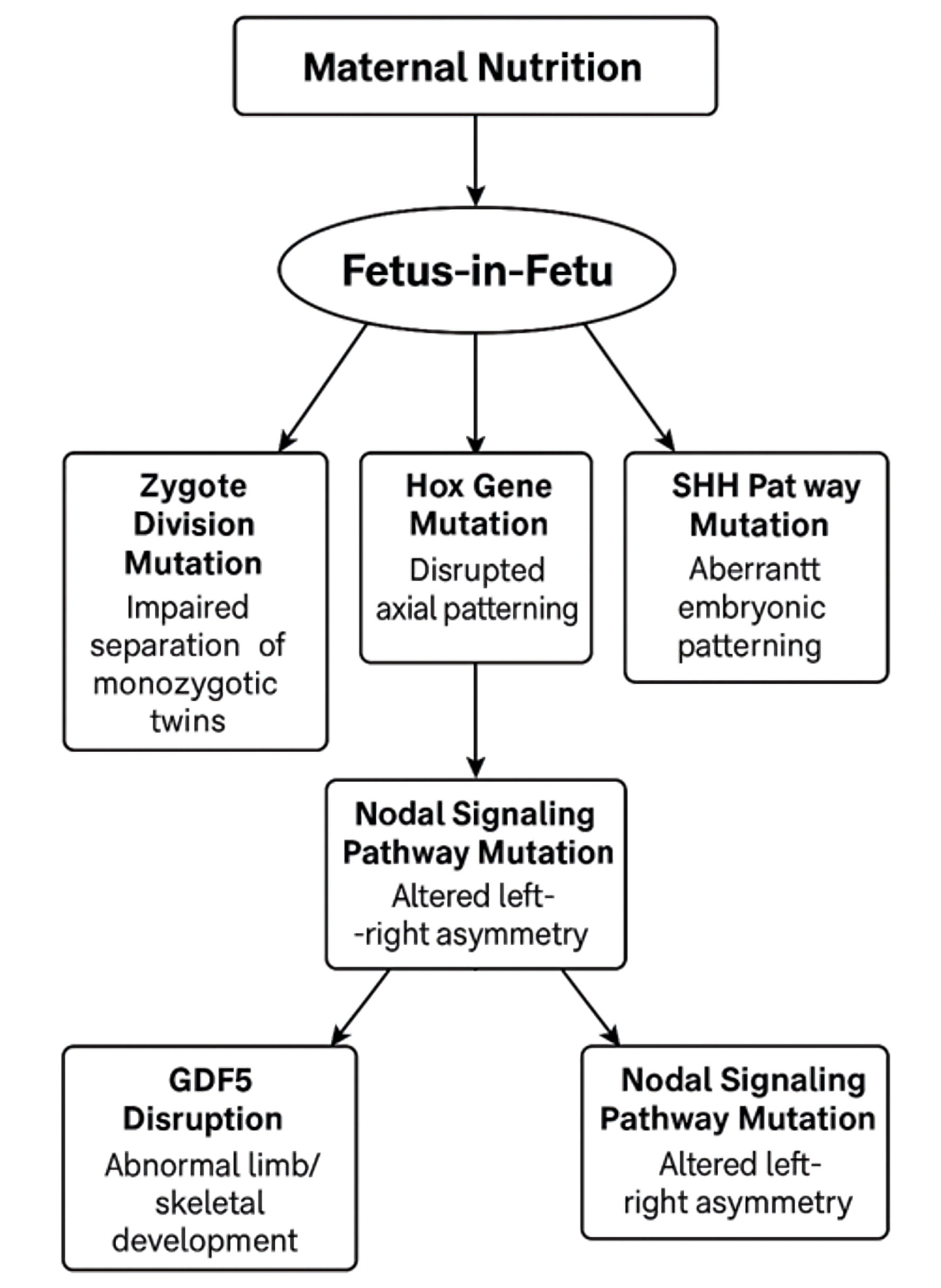
↓ Figure 3. Conceptual genetic and developmental signaling framework proposed for fetus-in-fetu (FIF). This figure presents a conceptual framework summarizing developmental signaling pathways that have been hypothesized to contribute to the formation of FIF based on indirect evidence from embryology, monozygotic twinning biology, and reported genetic analyses in affected cases. The pathways shown, including disruptions in zygotic separation, axial patterning genes such as Hox, and key embryonic signaling cascades including Sonic Hedgehog (SHH) and Nodal, are not established causal mechanisms but represent biologically plausible contributors to asymmetric twin development. Maternal nutritional influences are illustrated as a modifying background factor rather than a direct etiologic driver, reflecting theoretical modulation of early embryonic signaling rather than proven causation.
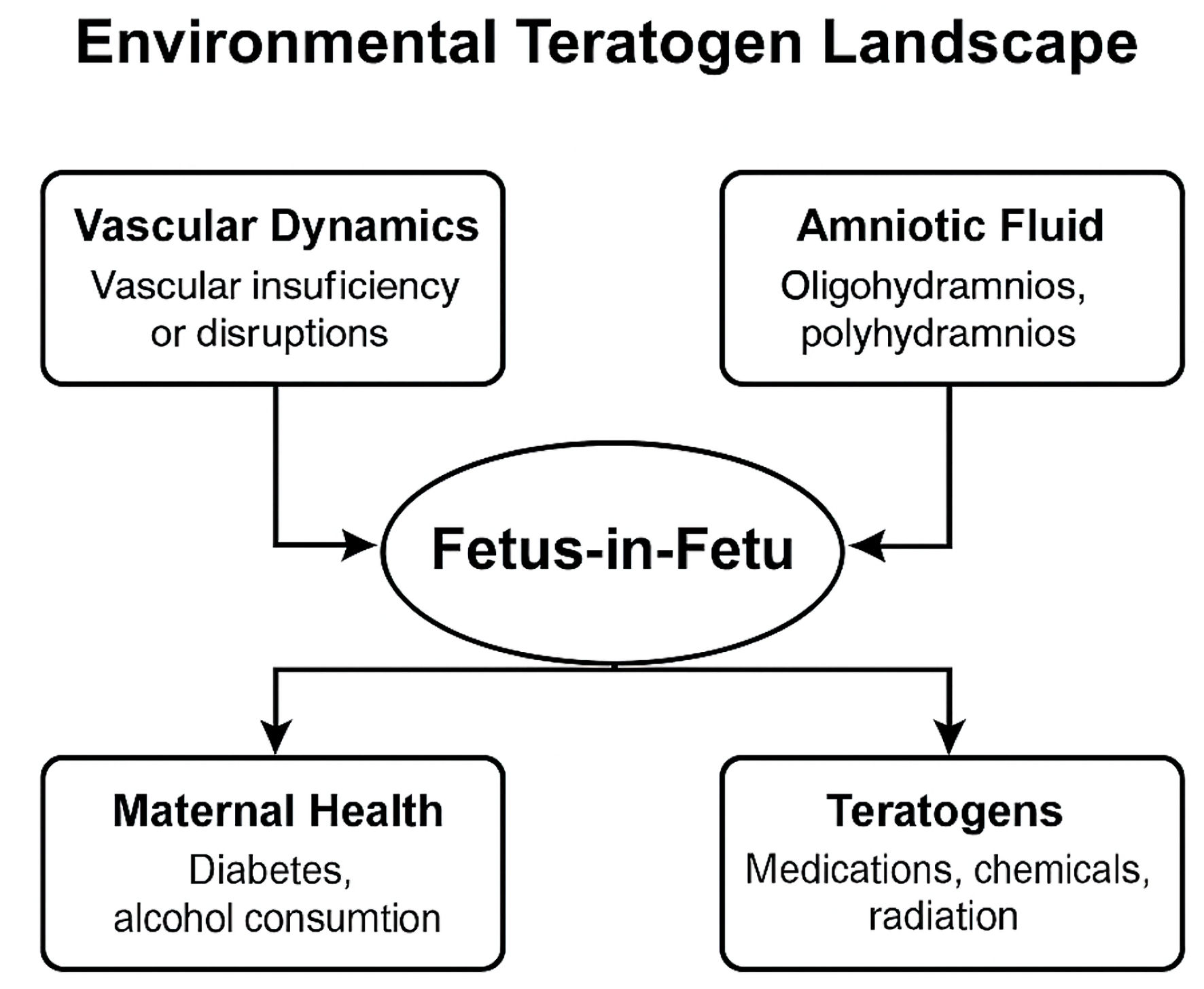
↓ Figure 4. Conceptual overview of environmental and maternal factors discussed in relation to fetus-in-fetu (FIF). This figure depicts environmental and maternal factors that have been discussed in the literature as theoretical modifiers of early embryonic development in cases of FIF. The elements shown, including vascular dynamics, amniotic fluid abnormalities, maternal health conditions, and external teratogenic exposures, are not established causal risk factors but represent hypotheses proposed to contextualize asymmetric monozygotic twin development. The diagram is intended as a conceptual synthesis rather than evidence of direct etiologic relationships, reflecting the current absence of consistent epidemiologic or experimental data linking environmental exposures to FIF.
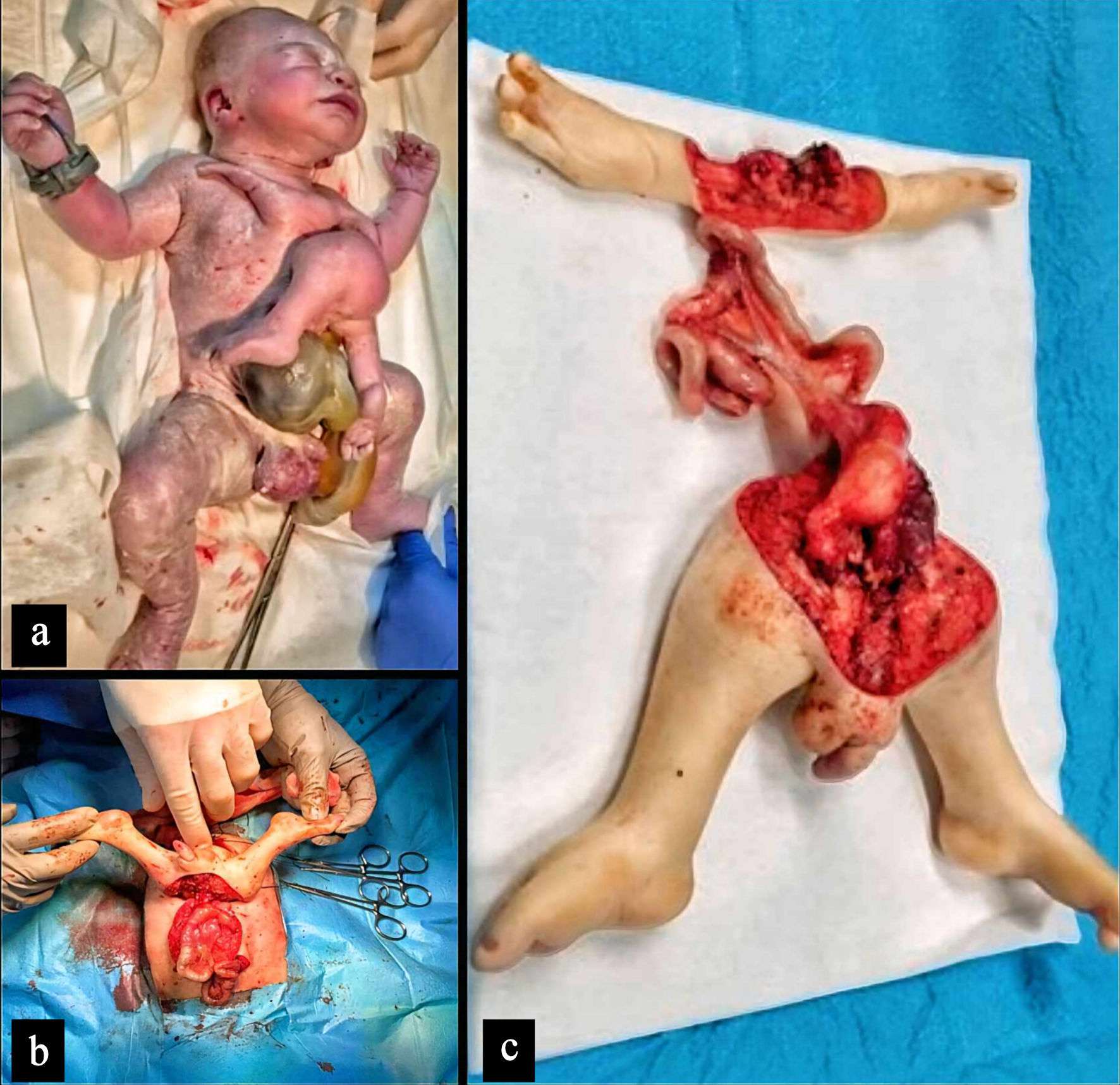
↓ Figure 5. Clinical and operative documentation of fetus-in-fetu (FIF) in a neonate with associated omphalocele. (a) Full-term male neonate immediately after birth demonstrating a large omphalocele with an externally visible parasitic FIF attached cranial to the abdominal wall defect. (b) Intraoperative photograph obtained during staged surgical excision, illustrating organized anatomical structures of the parasitic twin and shared vascular attachments to the host. (c) Resected FIF specimen following complete removal, showing well-differentiated limbs, external genitalia, and identifiable visceral components. Histopathological examination confirmed the presence of mature cartilaginous tissue, neural elements, and gastrointestinal structures, supporting the diagnosis of FIF rather than teratoma. All images were obtained with parental informed consent and anonymized according to institutional ethical standards; scale is inferred from surgical context.
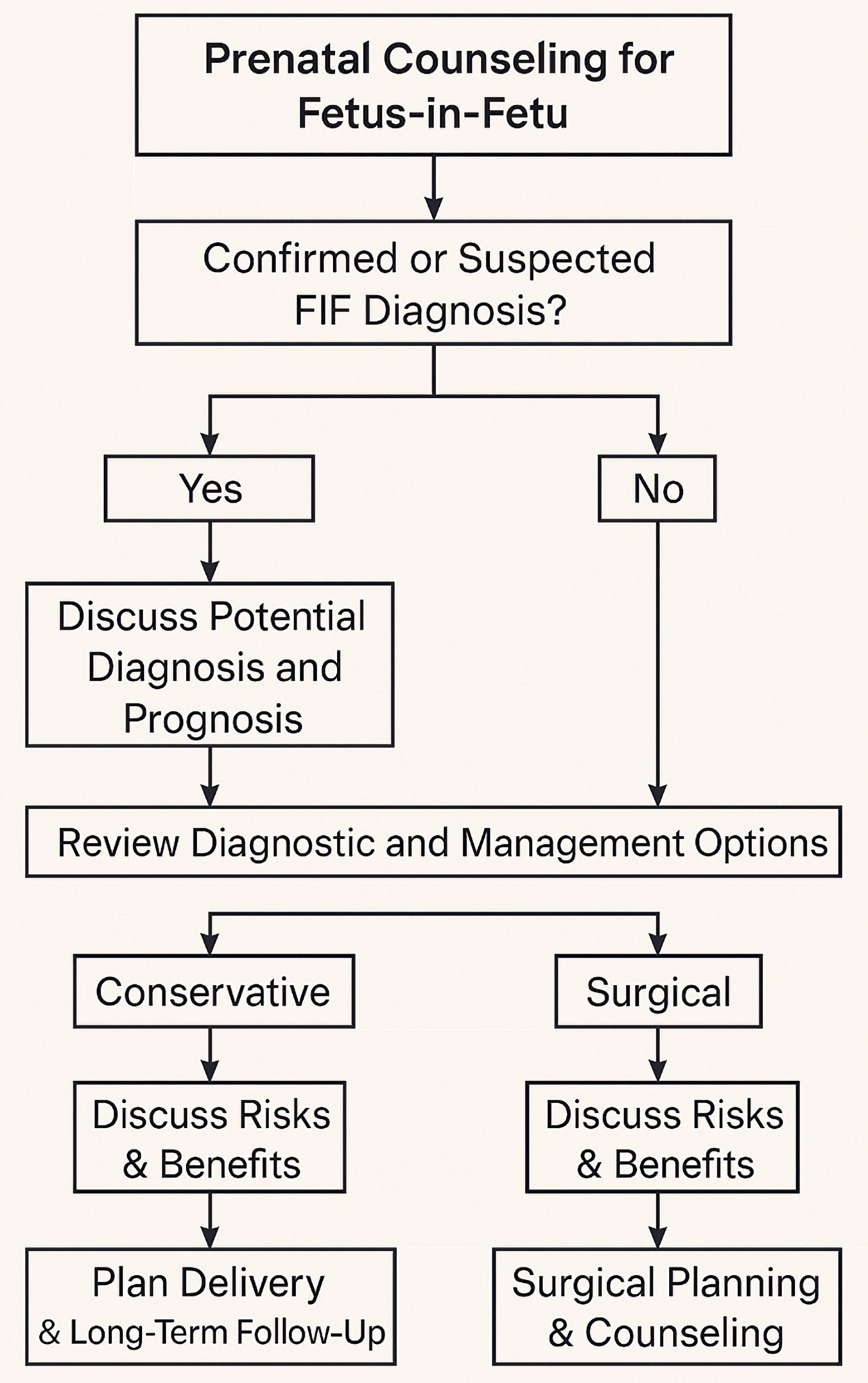
↓ Figure 6. Conceptual prenatal counseling pathway for suspected or confirmed fetus-in-fetu (FIF). This schematic illustrates a structured, non-directive counseling pathway commonly used in clinical practice when FIF is suspected or confirmed prenatally. The diagram integrates diagnostic confirmation through imaging, anticipatory counseling regarding prognosis and potential complications, and discussion of conservative versus surgical management pathways, with decisions guided by gestational age, anatomical complexity, and maternal–fetal condition. The pathway represents a synthesized clinical framework rather than a formal guideline and is intended to support shared decision-making that incorporates medical, ethical, and cultural considerations.
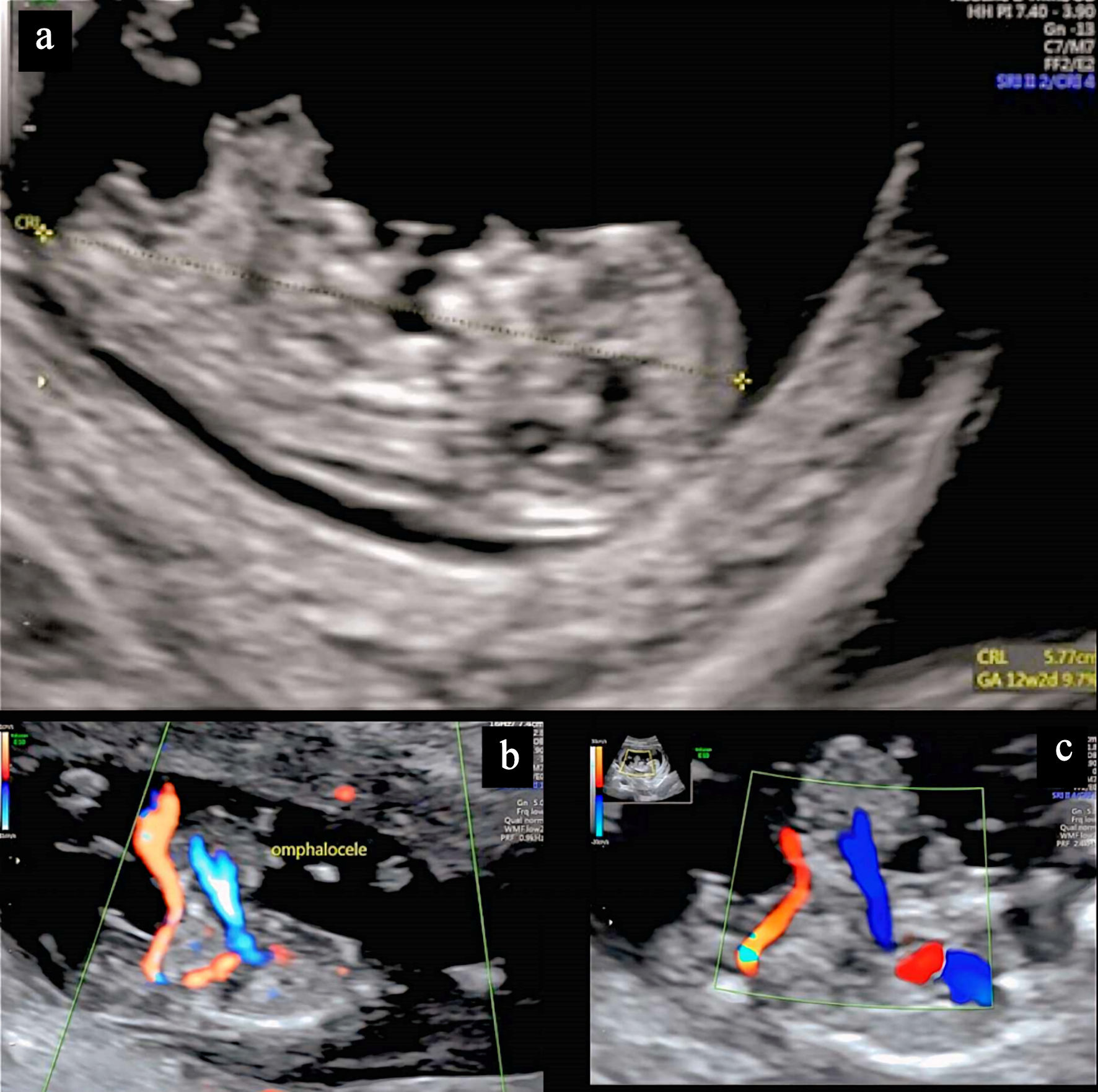
↓ Figure 7. First-trimester ultrasonographic findings with retrospective indicators of fetus-in-fetu (FIF). (a) Standard two-dimensional ultrasound image obtained at 12 + 2 weeks of gestation demonstrates a structurally developed fetus with a large omphalocele and a suspected cardiac anomaly; at the time of examination, FIF was not suspected. (b) Color Doppler imaging shows umbilical vessels supplying the omphalocele. Immediately cranial to the defect, an irregular echogenic area is visible, which was retrospectively recognized as corresponding to the parasitic FIF. (c) Focused color Doppler view further delineates vascular flow within the omphalocele, while the adjacent region harboring the parasitic structure remains partially obscured by overlapping anatomy and complex associated anomalies. This figure illustrates the diagnostic challenges of early gestational imaging in FIF and highlights how subtle sonographic findings may only become apparent upon retrospective review. Relative scale is inferred from standard first-trimester ultrasound acquisition parameters.
↓ Figure 8. Preoperative three-dimensional computed tomography (CT) of fetus-in-fetu (FIF) with associated omphalocele. Three-dimensional reconstructed CT image of a neonate obtained shortly after birth demonstrates a large omphalocele arising from the lower abdominal wall. Immediately cranial to the defect, a well-formed lower limb belonging to a parasitic FIF is seen emerging from the anterior torso of the host. The parasitic limb exhibits clear skeletal alignment and surrounding soft tissue consistent with organized musculoskeletal development. This imaging modality was essential for delineating anatomical relationships between the parasitic structures, abdominal wall defect, and host viscera, and it informed staged surgical excision and abdominal wall reconstruction. Image orientation and relative scale are inferred from standard neonatal CT acquisition parameters.

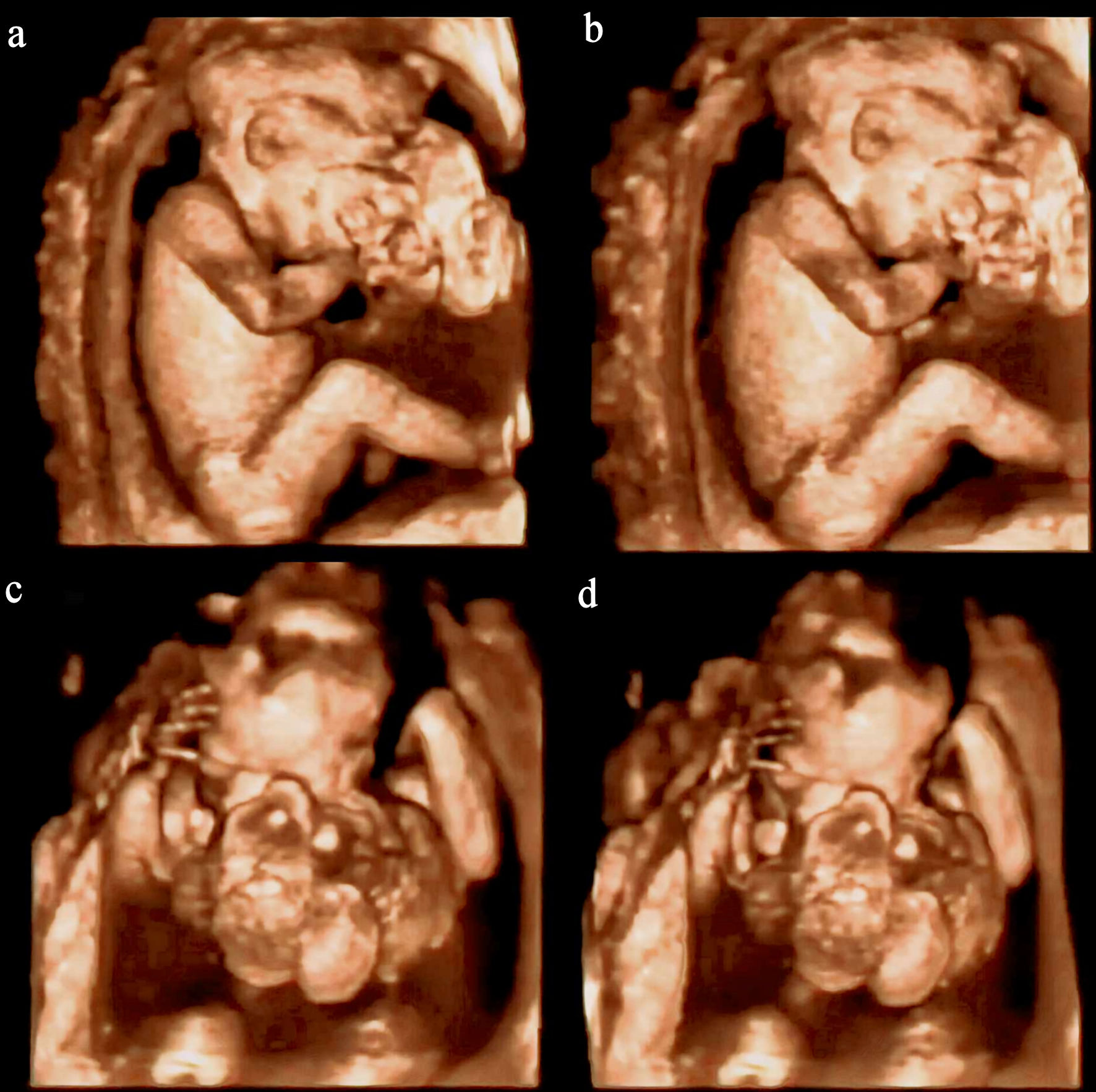
↓ Figure 9. Second-trimester three-dimensional ultrasonography of a craniofacial fetus-in-fetu (FIF). (a, b) Lateral three-dimensional ultrasound views obtained during the second trimester demonstrate a fetus with a large, irregular mass arising from the facial region, initially raising suspicion for a craniofacial tumor. Detailed surface rendering reveals organized internal contours suggestive of segmented structures and rudimentary limb elements within the mass. (c, d) Frontal three-dimensional views further delineate a partially organized parasitic twin attached at the midface, with bulbous cranial components and incomplete bilateral symmetry. This case, derived from previously reported clinical imaging in the literature, illustrates a rare craniofacial presentation of FIF and contrasts with the primary case described in this review, which lacks second- and third-trimester imaging. The images emphasize the diagnostic value of mid-gestation three-dimensional ultrasonography in distinguishing FIF from craniofacial neoplasms and in facilitating anticipatory perinatal planning, particularly with respect to airway management. Relative scale is inferred from standard fetal biometric acquisition.
Tables
↓ Table 1. Study Characteristics and Narrative Methodological Appraisal of Core Literature Included in the Review of Fetus-in-Fetu (FIF)
| Author | Study type/design | Population/setting | Sample size | Method | Primary objective | Key findings | Limitations | Risk of bias |
|---|
| This table includes all 25 core studies selected for qualitative synthesis in this review. Owing to the rarity of fetus-in-fetu, the available evidence consists predominantly of single case reports and small case series. Risk of bias was assessed narratively based on diagnostic certainty, completeness of reporting, and internal consistency rather than formal scoring tools. No study was excluded solely on the basis of methodological limitations. STR: short tandem repeat. |
| Lewis et al, 1961 [3] | Case report + analysis | Pediatric patient, UK | 1 | Clinical and pathology analysis | Differentiate FIF from teratoma | Introduced axial skeleton criterion | Pre-modern imaging | Moderate |
| Grant et al, 1969 [1] | Case report | Neonate, Australia | 1 | Surgical and pathological description | Describe clinical features of FIF | Early formal clinical characterization of FIF | Limited diagnostic tools | Moderate |
| Kakizoe et al, 1972 [23] | Case report | Neonate | 1 | Surgical findings | Describe scrotal FIF | Rare location | Single case | Moderate |
| Heifetz et al, 1988 [15] | Case series | Pediatric patients | 5 | Pathological analysis | Argue teratomatous origin | Challenged twin theory | Conceptual bias | Moderate |
| Eng et al, 1989 [4] | Case report | Infant, Taiwan | 1 | Imaging and histopathology | Correlate imaging with pathology | Demonstrated organized fetal structures | Single case | Moderate |
| Senyuz et al, 1992 [24] | Case report | Pediatric patient | 1 | Operative findings | Differentiate epignathus | Clarified oral cases | Single case | Moderate |
| Hing et al, 1993 [14] | Case report + genetics | Pediatric patient | 1 | STR analysis | Assess monozygotic origin | Genetic proof of twinning | Single case | Low–Moderate |
| Kim et al, 1993 [16] | Case report | Pediatric patient | 1 | Longitudinal imaging | Describe postnatal growth | Documented growth | Single case | Moderate |
| Chen et al, 1997 [10] | Case report | Prenatal diagnosis | 1 | Ultrasound, genetics | Assess prenatal diagnosis | Early prenatal confirmation | Limited follow-up | Moderate |
| Hanquinet et al, 1997 [13] | Case report | Pediatric patient | 1 | US and MRI | Compare FIF and teratoma | Imaging differentiation | Single case | Moderate |
| Sanal et al 1997 [25] | Case report | Neonate | 1 | Imaging and surgery | Report associated anomalies | Highlighted malformations | Single case | Moderate |
| Hopkins et al, 1997 [9] | Case report | Pediatric patient | 1 | Long-term follow-up | Report malignant recurrence | Demonstrated malignant potential | Exceptional case | Moderate |
| Fowler, 1998 [21] | Case report | Pediatric patient | 1 | Surgical exploration | Describe split notochord variant | Expanded spectrum | Atypical | Moderate |
| Thakral et al, 1998 [22] | Case report | Pediatric patient | 1 | Imaging and pathology | Review features | Confirmed markers | Narrative | Moderate |
| Hoeffel et al, 2000 [2] | Case series + review | Pediatric patients, France | 87 | Imaging and surgical review | Establish diagnostic criteria | Defined imaging and pathological hallmarks | Retrospective aggregation | Moderate |
| Shirani et al, 2005 [5] | Case report | Neonate | 1 | Operative and neurologic assessment | Describe parasitic twinning | Expanded anomaly spectrum | Not classic FIF | Moderate |
| Karaman et al, 2008 [7] | Case series | Pediatric patients | 2 | Surgical management | Report clinical presentation | Confirmed favorable outcomes | Small sample | Moderate |
| Tofigh et al, 2008 [8] | Case report | Pediatric patient | 1 | Imaging and surgery | Document rare presentation | Supported embryologic origin | Single case | Moderate |
| Khalifa et al, 2008 [17] | Case report | Pediatric patient | 1 | Clinical and surgery | Describe diagnostic process | Reinforced imaging diagnosis | Single case | Moderate |
| Gupta et al, 2010 [19] | Case report | Neonate | 1 | Clinical imaging | Document congenital anomaly | Supported definition | Single case | Moderate |
| Sharma et al, 2012 [18] | Case report | Pediatric patient | 1 | Imaging and surgery | Report rare anomaly | Typical presentation | Limited novelty | Moderate |
| Has et al, 2013 [12] | Case report | Prenatal setting | 1 | Prenatal ultrasound | Assess prenatal detection | Improved early diagnosis | Limited window | Moderate |
| Huang et al, 2013 [20] | Case report | Pediatric patient | 1 | Radiologic assessment | Report unusual presentation | Expanded phenotype | Single case | Moderate |
| Sitharama et al, 2017 [6] | Case report + review | Pediatric patient | 1 | Imaging and review | Review embryology and diagnosis | Clarified differential diagnosis | Narrative synthesis | Low–Moderate |
| Kumar et al, 2019 [11] | Case report | Adult patient | 1 | Imaging and surgery | Adult FIF presentation | Delayed diagnosis | Single case | Moderate |
↓ Table 2. Embryological Timeline and Proposed Developmental Disruptions Associated With Fetus-in-Fetu (FIF)
| Embryonic stage (day/post-fertilization) | Developmental event | Potential disruption leading to FIF |
|---|
| This table presents a conceptual synthesis of embryological stages relevant to FIF, informed by recurring observations in the reviewed literature and established principles of human embryology. It does not represent direct data extraction from individual studies, as no single report captures the complete developmental sequence. The proposed disruptions reflect plausible mechanisms inferred from clinical, imaging, and pathological findings. This framework is intended to aid interpretation rather than to assert definitive causality. |
| Day 1–3 | Fertilization and initial cleavages of zygote | Not applicable; monozygotic twinning has not yet occurred |
| Day 4–8 | Blastocyst formation and early monozygotic twinning (dichorionic diamniotic possible) | Too early for FIF formation; may lead to separate twins |
| Day 8–13 | Monochorionic monoamniotic twin formation; splitting of inner cell mass | Inclusion of one twin into the body of the other due to abnormal implantation or folding |
| Day 13–15 | Gastrulation and primitive streak formation | Asymmetric incorporation of one twin; axial development initiates inside host |
| Day 16–21 | Neurulation and early organogenesis; somite formation | Formation of vertebral axis and limb buds in parasitic twin; early differentiation within host embryo |
| Day 22–28 | Cardiac looping, gut tube formation, and neural crest migration | Limited or failed development of cardiovascular and nervous structures in parasitic twin |
| Week 5–8 | Organogenesis continues; limb and external genitalia become visible | Differentiation halts due to vascular insufficiency; structural organs remain rudimentary |
| Week 9–12 | Fetal period begins; rapid growth and functional maturation | Parasitic twin remains encapsulated; host circulation dominates; growth suppressed |
↓ Table 3. Genetic and Environmental Factors Implicated in the Development of Fetus-in-Fetu (FIF)
| Category | Factor | Evidence | Implication |
|---|
| This table represents a conceptual synthesis of genetic and environmental factors discussed across the reviewed literature and informed by established embryological principles. The listed factors reflect proposed mechanisms inferred from clinical, imaging, pathological, and molecular observations rather than definitive causal relationships. No consistent environmental or inherited genetic triggers have been empirically confirmed for FIF. STR: short tandem repeat. |
| Genetic | Monozygotic twinning (monochorionic diamniotic origin) | STR analysis and karyotyping confirm shared genotype between host and parasitic twin | Strong support for included twin theory; not a neoplastic origin |
| Genetic | Normal diploid karyotype | Consistent findings in parasitic twin tissue across multiple studies | Helps distinguish FIF from teratomas, which may show aneuploidy or mosaicism |
| Genetic | No inherited mutation patterns | Lack of familial recurrence; no consistent mutation profile identified | FIF is likely a sporadic developmental error, not a heritable condition |
| Genetic | Epigenetic dysregulation | Hypothesized based on asymmetric differentiation despite identical genomes | Could explain why a parasitic twin fails to fully develop |
| Genetic | Zygote division mutation | Impairment in the zygotic division process leads to incomplete separation during monozygotic twinning | Results in the internalization of one twin and development of a parasitic fetus |
| Genetic | Hox gene mutation | Disruptions in Hox genes, which control body plan and axial patterning, may lead to abnormal segmentation of the parasitic twin | Disruption of normal body axis formation and incomplete development of the parasitic twin |
| Genetic | Sonic Hedgehog (SHH) pathway mutation | Disruptions in SHH signaling interfere with embryonic patterning, particularly limb and axial development | Results in asymmetric development and improper internalization of the parasitic twin |
| Genetic | Nodal signaling pathway mutation | Disruptions in Nodal signaling affect left-right patterning, potentially leading to abnormal asymmetry in twin positioning | Affects the positioning and development of the parasitic twin within the host |
| Genetic | Growth and differentiation factor 5 (GDF5) disruption | Disruptions in GDF5, involved in limb and skeletal patterning, may cause incomplete or arrested development of the parasitic twin | Leads to underdeveloped limbs or axial structures in the parasitic fetus |
| Environmental | Vascular supply disruption | Parasitic twin depends entirely on the host’s circulation; poorly perfused structures noted | May contribute to arrested organ development and asymmetry |
| Environmental | Abnormal amniotic cavity dynamics | Theoretical link to spatial entrapment of a parasitic twin within host embryo | Could play a role in internalization of twin during folding process |
| Environmental | Placental anastomoses | Shared vascular connections observed in some prenatal FIF diagnoses | May facilitate twin inclusion or maintain parasitic growth |
| Environmental | No clear association with teratogens or maternal illness | Epidemiologic data fail to support any consistent external trigger | Reinforces FIF as a non-environmentally induced anomaly |
↓ Table 4. Commonly Accepted Diagnostic Markers and Modalities Used in the Evaluation of Fetus-in-Fetu (FIF)
| Category | Marker/feature | Modality | Diagnostic relevance |
|---|
| This table summarizes diagnostic markers and investigative modalities that are consistently described across reported cases of FIF and widely used in clinical practice. The listed features reflect convergent imaging, genetic, and histopathological criteria rather than outcomes from comparative or prospective studies. Diagnostic relevance is based on cumulative clinical experience and repeated observations in the literature. STR: short tandem repeat; β-hCG: beta human chorionic gonadotropin; CT: computed tomography; MRI: magnetic resonance imaging; PCR: polymerase chain reaction. |
| Imaging | Axial vertebral column | CT, MRI, prenatal ultrasound | Gold standard feature distinguishing FIF from teratoma; indicates embryonic origin |
| Imaging | Organized limb buds and symmetry | CT, MRI | Supports diagnosis of parasitic twin; shows structured development |
| Imaging | Encapsulated mass with cystic and solid components | Ultrasound, CT | Suggests inclusion phenomenon within host body; often seen in retroperitoneum |
| Genetic | Identical STR profile to host | Molecular genetics (PCR, STR analysis) | Confirms monozygotic origin; excludes neoplastic (teratomatous) origin |
| Genetic | Normal diploid karyotype | Karyotyping | Helps differentiate FIF from teratomas, which may show chromosomal abnormalities |
| Histopathology | Presence of vertebral elements and multi-organ tissues | Microscopic examination | Definitive confirmation; distinguishes from disorganized teratomatous growth |
| Tumor markers | Low or normal alpha-fetoprotein (AFP) | Serum analysis | Helps rule out yolk sac tumors or malignant germ cell tumors |
| Tumor markers | Negative β-hCG | Serum analysis | Further differentiates from certain teratomatous malignancies |
↓ Table 5. Conceptual Clinicopathological Comparison of Fetus-in-Fetu (FIF), Mature Teratoma, and Parasitic Twin
| Feature | FIF | Mature teratoma | Parasitic twin |
|---|
| This table provides a conceptual comparison based on recurrent clinicopathological features described across reported cases and established diagnostic criteria. The distinctions shown reflect consensus patterns used in clinical practice rather than results from comparative or prospective studies. The table is intended to aid diagnostic reasoning and differential classification, not to imply absolute or universal boundaries between entities. |
| Presence of axial skeleton | Yes | No | Yes |
| Bilateral symmetry | Yes | No | Often |
| Encapsulated mass | Yes | Yes | No |
| Monozygotic origin | Yes | No | Yes |
| Organ primordia | Yes | No | Yes |
| Disorganized germ layers | No | Yes | No |
| Malignancy potential | Rare | Possible | No |
| External attachment | No | No | Yes |
| Shared vasculature with host | Rare | No | Yes |
| Functional limbs/organs | Rare | No | Yes |