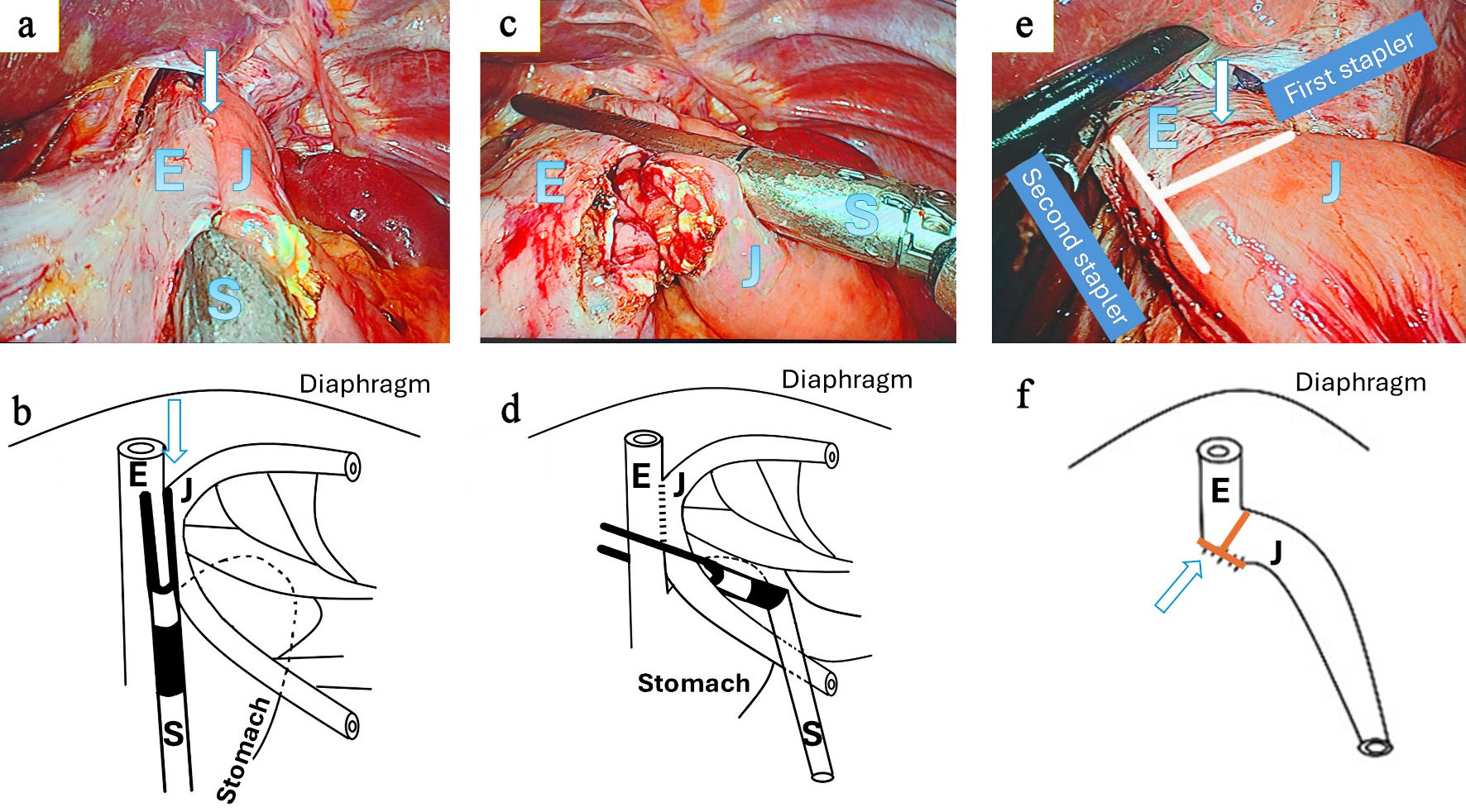
↓ Figure 1. Intracorporeal T-shaped functional end-to-end esophagojejunostomy. (a, b) Creation of the initial side-to-side esophagojejunostomy. Small enterotomies are made on the lateral wall of the esophagus (E) and the antimesenteric border of the jejunum (J), followed by insertion and firing of a linear stapler (S) to create a functional side-to-side anastomosis (arrow). (c, d) Perpendicular stapling step. A second linear stapler is applied perpendicular to the initial staple line, incorporating both the esophageal and jejunal walls at the level of the common entry hole. Upon firing, this step closes the common entry hole and trims the overlapping tissue edges rather than resecting the anastomosis. (e, f) Final configuration of the T-shaped functional end-to-end esophagojejunostomy. The intersection of the two staple lines creates a characteristic T-shaped geometry (arrow), resulting in a straight luminal alignment without a residual blind pouch or jejunal stump. The apparent stump-like structure corresponds to the transverse staple line rather than a true jejunal stump. E: esophagus; J: jejunum; S: stapler.