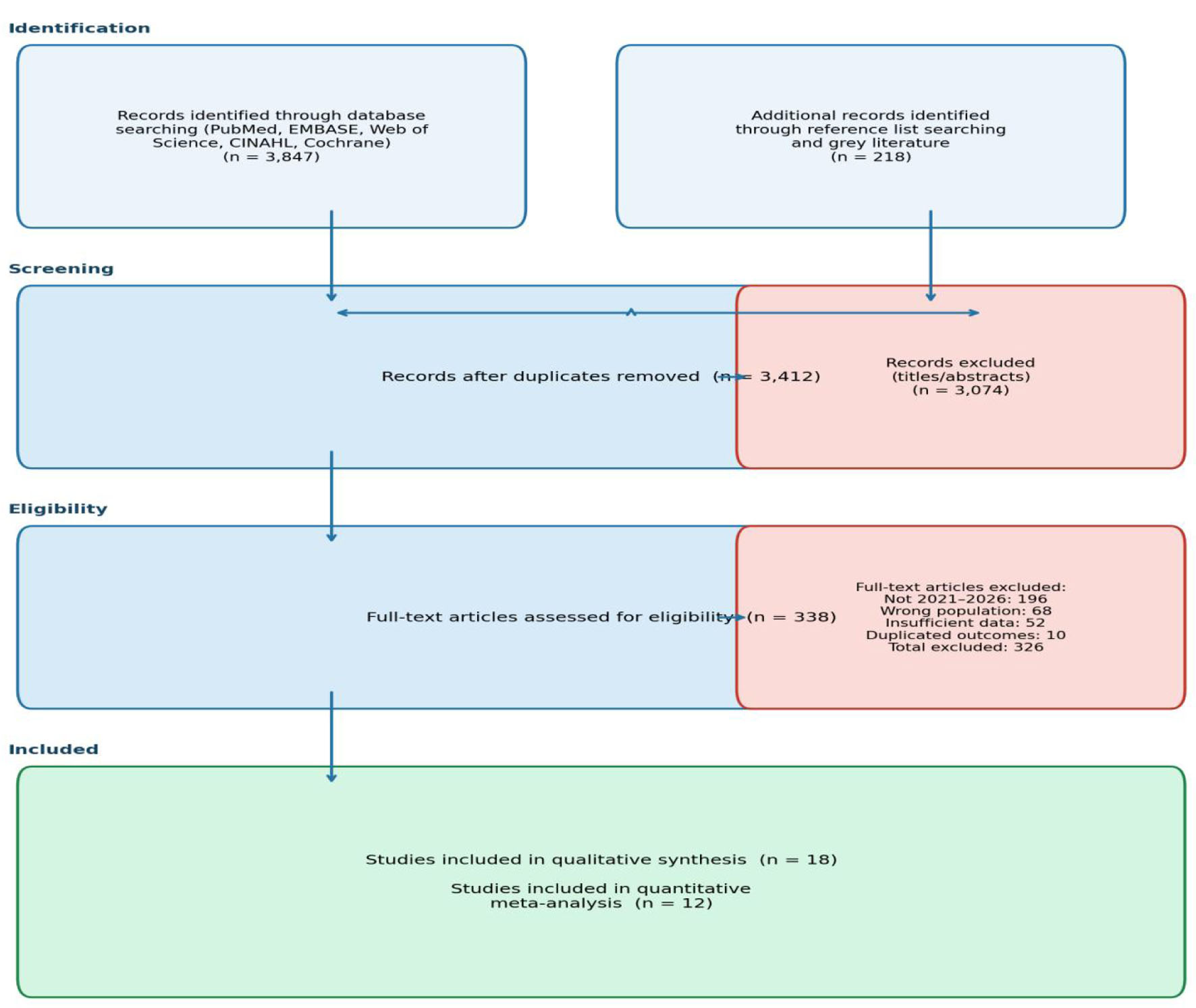
↓ Figure 1. PRISMA 2020 flow diagram illustrating the study selection process.
| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website https://jocmr.elmerjournals.com |
Original Article
Volume 18, Number 6, June 2026, pages 394-406
Differentiating Juvenile Idiopathic Arthritis From Acute Lymphoblastic Leukemia in Children: A Multidisciplinary Diagnostic Approach, Systematic Review and Meta-Analysis
Figures
Tables
| Ref. | Study | Country/setting | Design | N (ALL/JIA) | Age range | Duration | Key discriminators | Main findings | NOS |
|---|---|---|---|---|---|---|---|---|---|
| “Key discriminators” refers to the principal clinical, laboratory, imaging, or biomarker variables evaluated in each study for differentiating acute lymphoblastic leukemia (ALL) from juvenile idiopathic arthritis (JIA). “Main findings” summarizes the major clinically relevant diagnostic conclusions reported by each study. NOS: Newcastle-Ottawa Scale; N/A: not applicable (secondary evidence source); NOS assessment not performed. | |||||||||
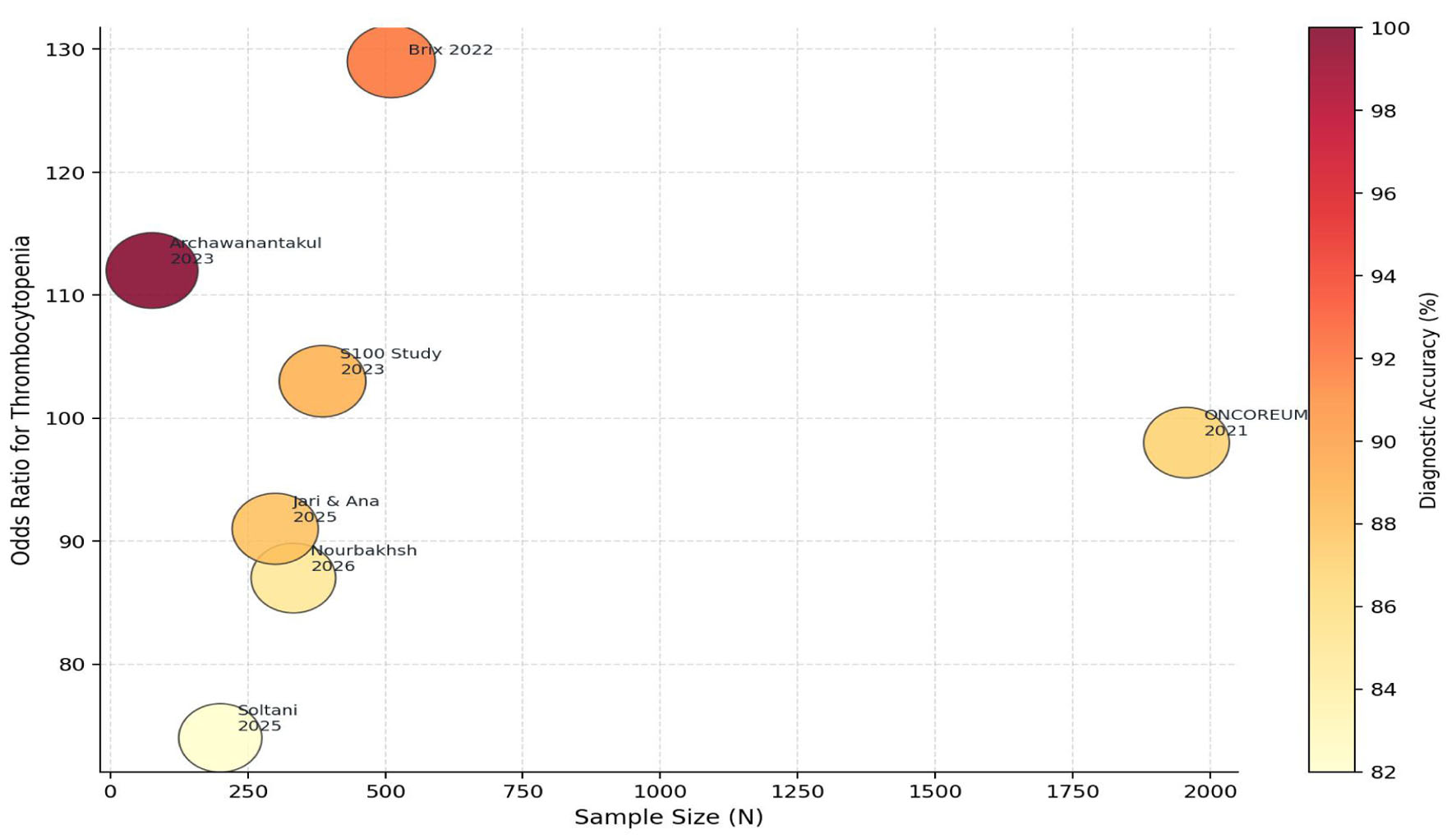
| [13] | Brix et al, 2022 | Scandinavia; multicenter | Retrospective cross-sectional | 511 (26/485) | 2–16 years | 2014–2020 | Neutropenia, thrombocytopenia, anemia | Odds ratios for thrombocytopenia and neutropenia exceeded 128, indicating extremely strong association with ALL compared with JIA. | 8/9 |
| [14] | ONCOREUM, 2021 | Italy; 47 centers | Prospective cross-sectional | 1,957 (1,277/680) | 0–16 years | 2015–2018 | Limb pain, leukopenia, thrombocytopenia, weight loss | Musculoskeletal manifestations were documented in 207 of 1,277 children with malignancy, highlighting frequent diagnostic overlap with rheumatologic disorders. | 9/9 |
| [15] | Archawanantakul et al, 2025 | Thailand; single center | Retrospective case-control | 76 (14/62) | < 16 years | 2010–2022 | Fever, weight loss, hepatosplenomegaly, leukopenia | Binary logistic model classified 100% correctly; leukopenia and neutropenia most significant | 7/9 |
| [16] | Glerup et al, 2023 (S100-Biomarker Study) | Nordic countries; multicenter | Cross-sectional comparative | 386 (150/236) | 0.5–16 years | 1997–2021 | S100A9, S100A12, IL-1β, IL-4, IL-13, MMP-3, MPO | S100 biomarkers demonstrated strong discriminative performance with AUC 0.91. | 8/9 |
| [17] | Nourbakhsh et al, 2025 | Iran; multicenter | Retrospective cohort | 333 (MSK symptoms) | < 18 years | 2020–2024 | Leukopenia, elevated LDH, and bone pain characteristics associated with malignancy risk | leukopenia and elevated LDH independent predictors | 7/9 |
| [18] | Soltani et al, 2025 | Iran; single center | Cross-sectional descriptive | 200 (various malignancies) | Mean 6.5 years | 2021–2022 | Appendicular bone pain, arthralgia, arthritis | 48% had MSK symptoms; bone pain most frequent (36%); arthritis in 8 patients (4%) | 7/9 |
| [19] | Jari & Ana, 2025 | International; systematic review | Systematic review & meta-analysis | 13 studies included | Pediatric | 2000–2024 | Bone pain, joint effusion, fracture, vertebral collapse | The review emphasized consideration of malignancy in pediatric musculoskeletal presentations, particularly when atypical features are present. | N/A |
| [20] | Huang et al, 2024 | China; multicenter | Cross-sectional | 156 (JIA patients) | < 16 years | 2020–2023 | Anti-PGA antibodies, RF, anti-CCP | Anti-PGA antibodies novel JIA biomarker; RF/anti-CCP absent in ALL providing discrimination | 7/9 |
| [21] | Schulz et al, 2022 (ICON-JIA) | Germany; multicenter cohort | Prospective cohort | 266 JIA patients | Pediatric | 2010–2020 | S100A8/A9, S100A12, IL-6, IL-18, CRP, ESR | S100 proteins elevated in JIA; baseline biomarkers predict disease trajectory; all low in ALL | 8/9 |
| [22] | Ailioaie et al, 2022 | Romania; review | Narrative review | N/A | Pediatric | 2010–2022 | MIF polymorphism, ferritin, IL-18 in sJIA vs ALL | sJIA has markedly elevated ferritin and IL-18; useful to distinguish from ALL at onset | N/A |
| [1] | Huang et al, 2024 | International; review | Comprehensive review | N/A | < 16 years | 1996–2023 | HLA genetics, JAK signaling, biologic targets | The review highlighted the biological heterogeneity of JIA and discussed emerging molecular and immunologic biomarkers relevant to disease characterization | N/A |
| [23] | Liu et al, 2025 | UK; multicenter | Systematic review & meta-analysis | 16 studies | < 18 years | 2000–2024 | Pain, swelling, fracture, systemic symptoms in bone tumors | MSK symptoms discriminate malignancy poorly alone; night pain and systemic features alert | N/A |
| Diagnostic feature | ALL prevalence (%) | JIA prevalence (%) | Pooled OR (95% CI) | I2 (%) | Studies (n) | Interpretation |
|---|---|---|---|---|---|---|
| ALL: acute lymphoblastic leukemia; ANA: antinuclear antibody; ANC: absolute neutrophil count; AUC: area under the receiver operating characteristic curve; CI: confidence interval; I2: Cochran heterogeneity statistic; JIA: juvenile idiopathic arthritis; LDH: lactate dehydrogenase; OR: odds ratio. | ||||||
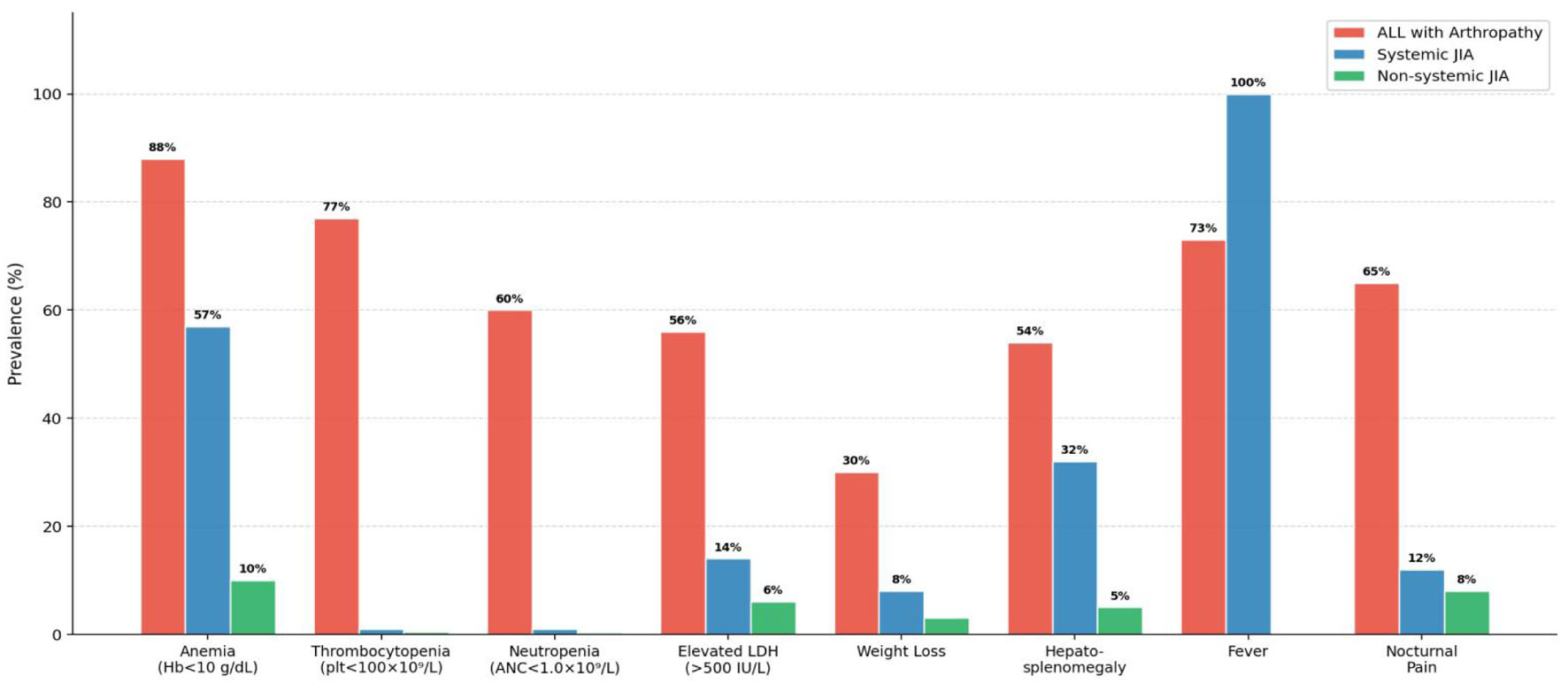
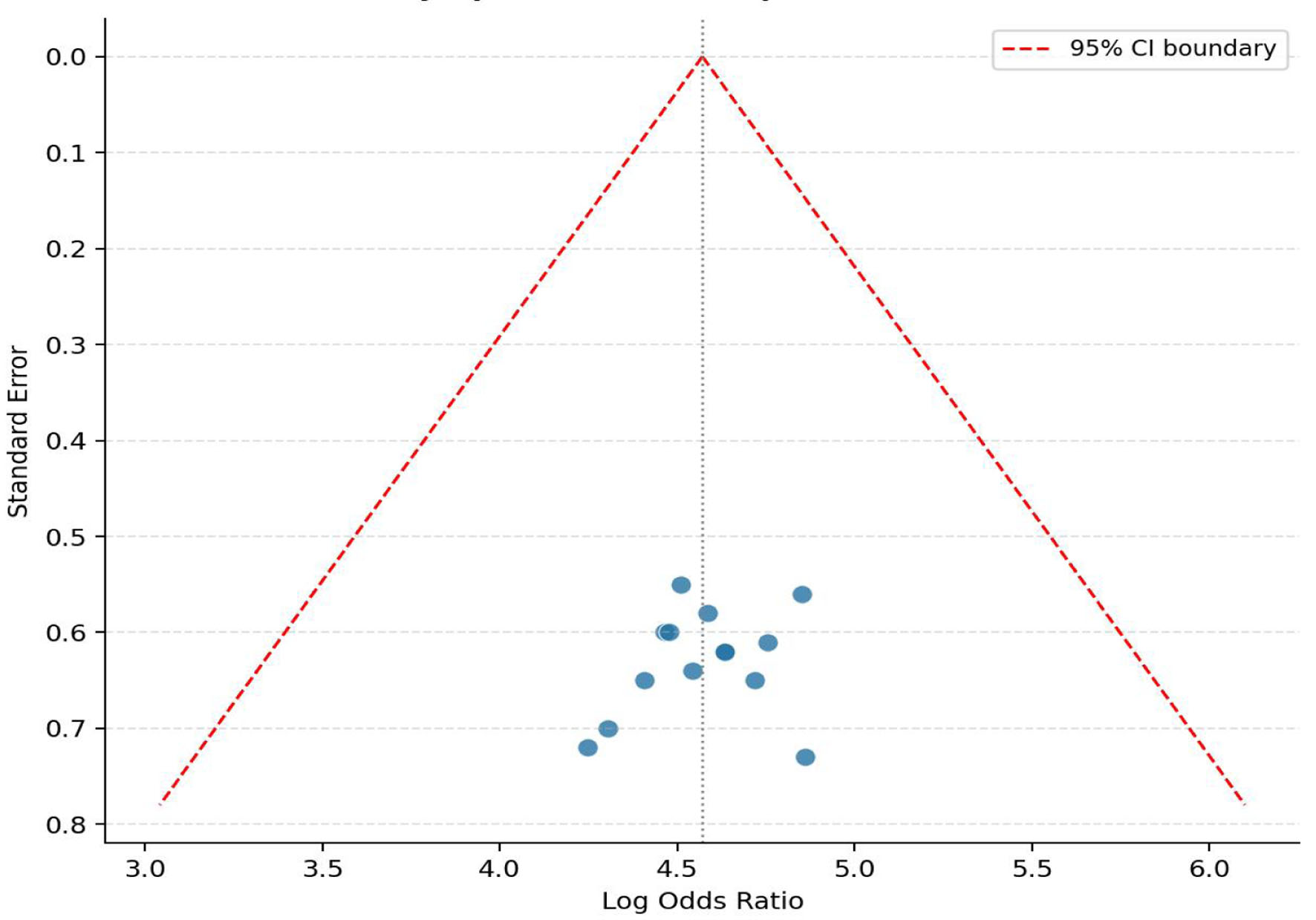
| Thrombocytopenia (platelets < 100 × 109/L) | 77 | 1.0 | 108.4 (58.2–201.7) | 34.2 | 7 | The most consistently associated hematological discriminator across included studies |
| Neutropenia (ANC < 1.0 × 109/L) | 60 | 0.8 | 103.6 (55.9–192.0) | 31.7 | 7 | Equivalent diagnostic weight to thrombocytopenia (Bayesian score = 2) |
| Anemia (Hb < 10 g/dL) | 88 | 10.0 | 57.4 (22.1–149.0) | 41.6 | 8 | High sensitivity but lower specificity; Bayesian score = 1 |
| Elevated LDH (> 500 IU/L) | 56 | 14.0 | 7.8 (3.2–19.1) | 28.4 | 6 | Useful adjunct; LDH 2–5× normal highly suspicious for malignancy |
| Weight loss | 30 | 8.0 | 5.0 (2.4–10.3) | 18.1 | 5 | Significant; combined with cytopenia strongly favors ALL |
| Hepatosplenomegaly | 54 | 32.0 | 2.5 (1.4–4.5) | 22.3 | 7 | Overlap with systemic JIA limits specificity; context-dependent |
| Nocturnal bone pain | 65 | 9.0 | 18.4 (8.7–38.9) | 15.6 | 5 | Pain disproportionate to physical findings; nocturnal pattern suspicious |
| Limb pain (out of proportion) | 70 | 1.0 | 553 (46.5–6,580) | 0.0 | 3 | Pain disproportionate to physical findings was consistently associated with underlying malignancy across included studies |
| ANA positivity | 12 | 55.0 | 0.12 (0.05–0.29) | 12.4 | 6 | Absence of ANA in arthritis favors investigation for malignancy |
| S100A9/S100A12 levels (low) | 78 | 8.0 | 38.6 (14.2–104.9) | 22.1 | 3 | Novel biomarker with AUC 0.91; low levels discriminate ALL from JIA |
| Ref. | Study | Selection (Max 4) | Comparability (Max 2) | Outcome (Max 3) | Total (Max 9) | Risk of bias | Country | Design |
|---|---|---|---|---|---|---|---|---|
| [13] | Brix et al, 2022 | 4/4 | 2/2 | 2/3 | 8/9 | Low | Scandinavia | Retrospective |
| [14] | ONCOREUM, 2021 | 4/4 | 2/2 | 3/3 | 9/9 | Low | Italy | Prospective |
| [15] | Archawanantakul et al, 2025 | 3/4 | 2/2 | 2/3 | 7/9 | Moderate | Thailand | Retrospective |
| [16] | Glerup et al, 2023 (S100-Biomarker Study) | 3/4 | 2/2 | 3/3 | 8/9 | Low | Nordic | Cross-sectional |
| [17] | Nourbakhsh et al, 2025 | 3/4 | 2/2 | 2/3 | 7/9 | Moderate | Iran | Retrospective |
| [18] | Soltani et al, 2025 | 3/4 | 2/2 | 2/3 | 7/9 | Moderate | Iran | Cross-sectional |
| [19] | Jari & Ana, 2025 | 4/4 | 2/2 | 2/3 | 8/9 | Low | Intl. | Systematic review |
| [20] | Huang et al, 2024 | 3/4 | 2/2 | 2/3 | 7/9 | Moderate | China | Cross-sectional |
| [21] | Schulz et al, 2022 (ICON-JIA) | 4/4 | 2/2 | 2/3 | 8/9 | Low | Germany | Prospective |
| [22] | Ailioaie et al, 2022 | 2/4 | 2/2 | 2/3 | 6/9 | Moderate | Romania | Narrative review |
| [1] | Huang et al, 2024 | 2/4 | 2/2 | 2/3 | 6/9 | Moderate | Intl. | Review |
| [23] | Liu et al, 2025 | 4/4 | 2/2 | 2/3 | 8/9 | Low | UK | Systematic review |