| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website https://jocmr.elmerjournals.com |
Original Article
Volume 16, Number 7-8, August 2024, pages 363-374

A Complex Interplay of Tumor Microenvironment Could Enhance Cholangiocarcinoma Progression Even After Surgery: A Prospective Study
Asmaa M. Zahrana, Amal Rayanb, Khaled Saadc, l, Khalid Rezkd, Ahmed Solimane, Mohamed Ahmed Rizke, Aya Mohammed Mahrosf, Essam-Eldeen M.O. Mahrang, Mohamed Ahmed Bashirh, Heba M. Elmasrya, Zeinab Albadry M. Zahrani, Ahmed Khalid Ibrahimj, Mohsen M. Fageehk, Doaa A. Gamalb
aClinical Pathology Department, South Egypt Cancer Institute, Assiut University,
Assiut, Egypt
bClinical Oncology Department, Faculty of Medicine, Assiut
University, Assiut, Egypt
cPediatric Department, Faculty of Medicine, Assiut
University, 71516 Assiut, Egypt
dSurgical Oncology Department, South Egypt
Cancer Institute, Assiut University, Assiut, Egypt
eGeneral Surgery Department,
Faculty of Medicine, Assiut University, Assiut, Egypt
fDepartment of Hepatology,
Gastroenterology, and Infectious Diseases, Kafrelsheikh University, Kafrelsheikh,
Egypt
gDepartment of Tropical Medicine and Gastroenterology, Faculty of
Medicine, New Valley University, New Valley, Egypt
hClinical Pathology
Department, Faculty of Medicine, Al-Azhar University, Assiut, Egypt
iClinical
Pathology Department, Faculty of Medicine, Assiut University, Assiut,
Egypt
jFaculty of Medicine, National Assiut University, Assiut,
Egypt
kDirector of forensic toxicology services, FMSC, Jazan, Saudi
Arabia
lCorresponding Author: Khaled Saad, Pediatric Department, Faculty of
Medicine, Assiut University, 71516 Assiut, Egypt
Manuscript submitted May 11, 2024, accepted July 12, 2024, published online July 23,
2024
Short title: PD-1+ Expression and Macrophage Level in CCA
doi:
https://doi.org/10.14740/jocmr5201
| Abstract | ▴Top |
Background: The current study was conducted to explore the impact of macrophages and programmed cell death protein 1 (PD-1) expression on tumor-infiltrating lymphocytes (TILs) on treatment outcomes and to define the interaction between these factors and the clinicopathologic features of advanced cholangiocarcinoma (CCA) patients.
Methods: Twenty-five patients with metastatic CCA were recruited for the current study from El-Rajhi Hospital and the Clinical Oncology Department of Assiut University. Additionally, 19 healthy controls were included. Before the flow cytometric detection of immune cells, the diagnosis and staging of CCA were performed based on surgical intervention, imaging, carbohydrate antigen 19-9 (CA19-9), and carcinoembryonic antigen (CEA) determinations. This was followed by flow cytometric detection of CD4+, CD8+, CD4+PD-1+, CD8+PD-1+, and CD11b+CD68+ macrophages in the peripheral blood of both patients and controls.
Results: The current results revealed higher levels of CD4+, CD8+, and CD11b+CD68+ macrophages in controls compared to patients. At the same time, PD-1 expression was significantly higher in patients compared to controls. CD4+ was correlated with improved progression-free survival (PFS), while CD8+PD-1 was associated with shorter PFS. In general, CD4+ and CD8+ levels progressively increased with improved response to treatments, differentiation, single organ site metastasis, and surgical interventions. On the contrary, PD-1 expression and macrophages progressively increased with worsening response, dedifferentiation, multiple organ sites, and surgical interventions. The median PFS was 12 months, and the mean ± standard error (SE) was 13.1 ± 1.3.
Conclusions: CCA has a desmoplastic microenvironment with complex immunologic topography and tumor-reactive stroma. The immune landscape of the peripheral blood mononuclear cells (PBMCs) in CCA patients before treatment could reflect the state of systemic immune function and response to treatments. Our results revealed that T-lymphocytes correlated with better prognosis while macrophages and PD-1+ expression were associated with poor outcomes.
Keywords: Cholangiocarcinoma; PD-1+ expression; Macrophages; PBMNCs; Progression-free survival
| Introduction | ▴Top |
Cholangiocarcinoma (CCA) is a heterogenous malignancy with aggressive behavior and a high death rate. Recently, its incidence has been rising worldwide [1]. The incidence is relatively low in high-income countries but rising, even up to 40 times higher, in some countries such as China and Korea; where infection with liver flukes is the most likely cause of CCA [2]. The risk of CCA is related to a variety of pathologic states such as infections (flukes, hepatitis C and hepatitis B viruses), cholestatic liver diseases, biliary stone diseases, metabolic disorders (diabetes, obesity, non-alcoholic fatty liver diseases), chemicals, toxins, and drugs. All these factors result in cholestasis, inflammation, and ultimately carcinogenesis [3, 4]. Data regarding its incidence in Egypt are lacking, but expected to be high and rising, due to high incidence of hepatic flukes and viral infections [5].
CCA is divided into extrahepatic and intrahepatic (iCCA) subtypes. The former is further divided into perihilar (pCCA) and distal (dCCA) subtypes with distinct biological, epidemiological, prognostic, and therapeutic challenges. The majority of patients have unresectable diseases at the time of presentation, with 50% of patients deemed potentially resectable at the time of diagnosis found to be unresectable or metastatic at the time of surgery [6], so the role of neoadjuvant chemotherapy appears to improve resectability and decrease postoperative recurrences.
Tumor cells secrete many factors and cytokines to recruit and shape various cell types in the tumor microenvironment (TME) to enhance tumor initiation and progression. These cells include tumor-associated macrophages (TAMs), tumor-infiltrating lymphocytes (TILs), Tregs, neutrophils, and natural killer (NK) cells [7, 8]. TAMs are derived mainly from blood monocytes rather than activated stromal cells (Kupffer cells), then recruited to CCA by releasing different factors, including vascular endothelial growth factor A (VEGF-A), monocyte chemoattractant protein-1(MCP-1), macrophage colony-stimulating factor-1 (CSF-1), and tumor necrosis factor-like weak inducer of apoptosis (TWEAK)/fibroblast growth factor-inducible 14 (Fn14) [9, 10].
MCP-1 enhances the recruitment of TAMs into CCA and the expression of the CD206+ marker after tumor infiltration. TAMs attain a protumor phenotype (M2) instead of their original proinflammatory and antitumor phenotype (M1) [10]. In addition to CD206+ TAMs, programmed cell death protein 1 (PD-1)+ TAMs are recruited into the CCA niche to facilitate tumor progression, resulting in poor clinical outcomes [11]. The interplay between TAMs and cancer stem cells (CSCs) is supported by high levels of CD163+ and CD206+ TAMs and CD44+ and EPCAM+ CSCs. CSCs are the spearhead for carcinogenesis, recurrence, metastasis, and drug resistance [12-14].
PD-1, referred to as CD279, is expressed on activated T, B, and NK cells, monocytes, macrophages, dendritic cells, and, more importantly, its expression on TILs [15]. Transcription of PD-1 is induced by nuclear factor of activated T cells (NFAT), NOTCH, forkhead box protein (FOX) O1 and interferon (IFN) regulatory factor 9 (IRF9), binding of PD-1 with its ligands PD-L1 and PD-L2 promotes T cell activation, proliferation, and disruption of antitumor immune response [16].
PD-1 inhibits both innate and adaptive immune responses; subsequently, accumulating evidence supports that its targeting promotes an antitumor response and clinical improvements in many cancer types [17]. On the other hand, there are conflicting results regarding the association of TAMs with the clinical behavior of CCA. Some studies indicated worse outcomes, while others reported better results [18]. Our study was conducted to explore the impact of macrophages and PD-1 expression on TILs on treatment outcomes, emphasizing the interaction between these factors and the clinicopathologic features of advanced CCA patients.
| Materials and Methods | ▴Top |
The study was conducted in full concordance with principles of the Declaration of Helsinki, Good Clinical Practice (GCP), and within the laws and regulations of Egypt. The nature of the study was clarified to all participants, and participants were assured that their confidentiality was protected. Participation was entirely voluntary, and they were able to withdraw at any time without providing a reason, and their data were destroyed if they wished; the study was approved by the Ethics Committee of Assiut University (Institutional Review Board (IRB) = 04-2023-300194). The researchers also fully explained the nature of the research at the start of the work, and informed written consent was obtained from all cases and controls.
Twenty-five patients were recruited for the current study from El-Rajhi Hospital and the Clinical Oncology Department of Assiut University. Only patients with metastatic CCA were recruited, performance status by ECOG < 2, ages > 18 and < 80 years, no previous chemotherapy or immunotherapy after being metastatic, those who received palliative radiotherapy were included; patients with a previous history of adjuvant chemotherapy treatments within 1 year before recruitment, and those with concurrent infections at the time of sampling were excluded. Also, 19 healthy controls were included to participate in the flow cytometric detection of PD-1 on immune cells and macrophages.
Preliminary diagnosis was suspected based on history and clinical examination (obstructive jaundice, abdominal pain, or attack of cholangitis), measurement of carbohydrate antigen 19-9 (CA19-9), and carcinoembryonic antigen (CEA). The diagnosis was confirmed by endoscopic retrograde cholangiopancreatography (ERCP) and biopsy, endoscopic ultrasound (EUS)-guided fine needle aspiration cytology (FNAC), tru-cut needle biopsy (TCNB), or after surgery.
Previous surgical interventions varied from palliative resection of the hepatic duct without adequate safety margin or lymph node dissection, palliative bypass, Whipple’s operation with partial pancreatectomy, second and third parts duodenectomy, and lymph node dissection for distal CCA. Also, previous hepatic resection for intrahepatic CCA was reported. Palliative percutaneous drainage of bile for inoperable lesions or stenting of the common bile duct by ERCP was done.
Before blood sampling and flow cytometry, the staging was done using magnetic resonance imaging (MRI) with contrast of abdominopelvis, multislice computed tomography (MSCT) of the chest, bone scan, blood chemistry, hemograms, and blood tumor markers (CA19-9 and CEA). All data were collected, followed by flow cytometric detection of CD4+, CD8+, PD-1 expression of T cells, and CD11b+CD68+ macrophages of peripheral blood. Two inflammatory parameters were calculated, including neutrophil to lymphocyte ratio (NLR) and mean platelet volume/platelet count ratio (MPR), followed by chemotherapy treatment.
Treatment of patients mainly consisted of systemic chemotherapy with gemcitabine-based regimens (gemcitabine and cisplatin, gemcitabine and capecitabine, and gemcitabine and oxaliplatin), or single agent gemcitabine or capecitabine. Some patients received palliative radiotherapy concurrently with capecitabine. After 4 - 6 months of treatments, those achieved a response were kept on follow-up without maintenance chemotherapy, and second-line treatments were resumed on progression.
Flow cytometric detection of macrophage and PD-1 expression on T cells
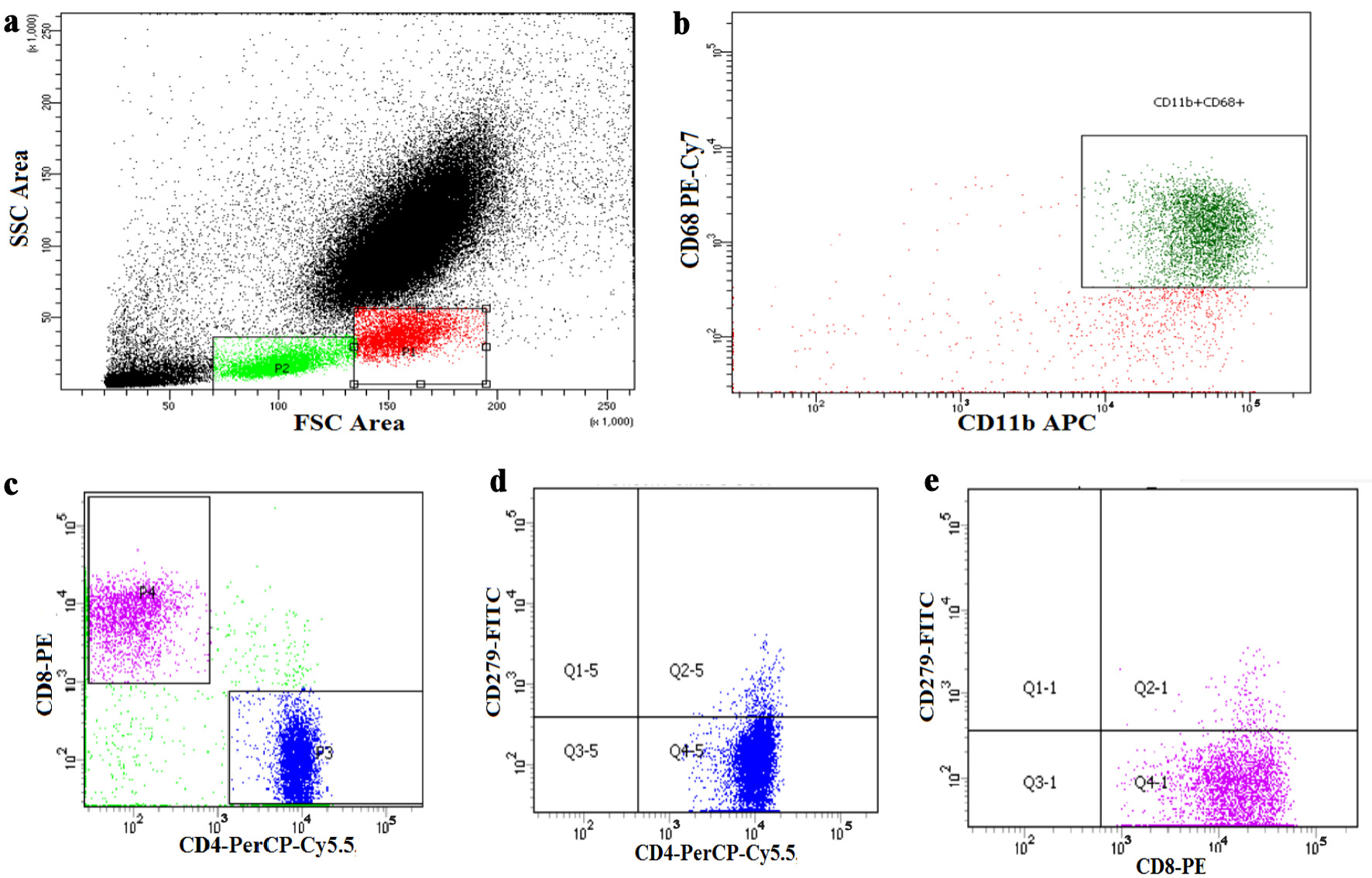
Peripheral blood was stained for 20 min with CD8-PE, CD4-PerCP-Cy5.5, CD279-FITC, CD68 PE-Cy7, and CD11b-ABC (Becton Dickinson Biosciences, CA, USA). After red blood cells (RBCs) lysis and washing, the cells were resuspended in phosphate-buffered saline (PBS) and analyzed using FACSCanto flow cytometry (BD Biosciences, USA). A forward and side scatter histogram was used to define the lymphocytes and monocytes (macrophage) population. Then, CD68 and CD11b were assessed on the monocyte population to detect total macrophage. CD4+ and CD8+ cells were also evaluated on lymphocytes and then gated for further analysis of the expression of CD279 (PD-1). The results were expressed as a percentage, as shown in Figure 1.
 Click for large image |
Figure 1. Flow cytometric detection of the checkpoint expression on T cells. (a) Forward and side scatter histogram was used to define monocytes and lymphocytes population. (b) CD68 and CD11b were assessed on the monocyte population to detect total macrophage. (c) Then CD4+ cells and CD8+ cells were assessed on lymphocytes and then gated. (d, e) The expression of CD279 (PD-1) was assessed on CD4+ and CD8+ cells. PD-1: programmed cell death protein 1. |
Statistics
Data were analyzed using IBM SPSS version 26 for descriptive stats; mean, median, standard deviation, and percentages were used for inferential stats, Mann Whitney U test for comparison between scale variables for two categories, and Robust tests (with correction of inhomogeneity of variances) and Kruskal Wallis test for more than two categories, Spearman rho correlation for relations between immune cells and survival, Kaplan-Meier test for graphing and calculation of progression-free survival (PFS) and overall survival. Results with P value < 5% were considered significant. PFS was calculated from the time of diagnosis of metastatic CCA to the time of death or progression. Multivariate analysis was done using Cox regression with the forward stepwise method.
| Results | ▴Top |
The current study involved 25 cases of metastatic CCA treated in the Clinical Oncology Department of Assiut University. Whether they were metastatic at presentation or metastatic at the time of relapse, the age, sex, and performance status of patients were tabulated (Table 1). The median age was 59 years; males were slightly more affected than females; nearly two-thirds of patients had a performance of 1 - 2; weight loss of > 5% was detected in 36% of patients. Almost all patients had hypertension, diabetes, or both; all females were non-smokers, while all males were either smokers or ex-smokers (Table 1).
 Click to view |
Table 1. Demographic Data of
Patients |
Extrahepatic CCA was reported in 80% of patients, while intrahepatic CCA in 20% of them. The commonest sites of metastasis were the peritoneum, liver, non-regional lymph nodes (LNs), and lungs. All intrahepatic CCA were mass-forming, most dCCAs were detected to have intraductal-growing tumors. Dedifferentiation was found in 44% of patients, and 52% of patients underwent surgery, whether radical or palliative. The overall response and locoregional control rates to gemcitabine-based combinations were 56% and 84%, respectively (Table 2).
Click to view |
Table 2. Clinicopathologic
Characteristics |
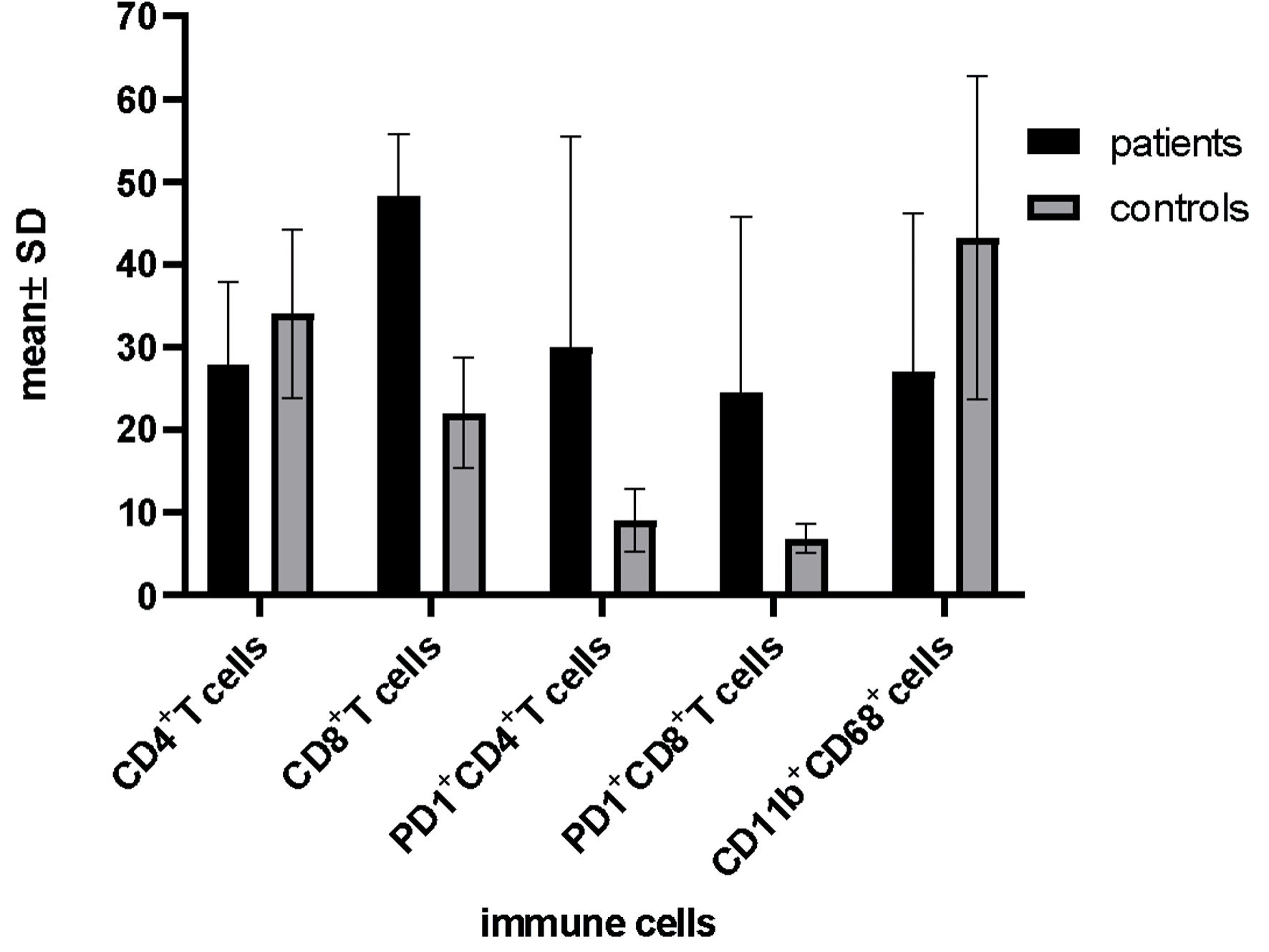
Regarding CD4+ and CD8+ cells, the mean percentages were higher for controls compared to patients but insignificant (27.9 ± 9.9 vs. 34.1 ± 10.2, P = 0.05, and 18.34 ± 7.5 vs. 22.1 ± 6.7, P = 0.09 for patients and controls, respectively). However, the expression of PD-1 on these cells was significantly higher in patients compared with controls (for CD4+: 30.04 ± 25.5 vs. 9.1 ± 3.8, P < 0.001. for CD8+: 24.6 ± 21.1 vs. 6.9 ± 1.8, P < 0.001, respectively). Regarding CD11b+CD68+ macrophages, they were significantly accumulated in controls compared with patients (27.1 ± 19.1 vs. 43.2 ± 19.5 for patients and controls, respectively, P = 0.008) (Fig. 2).
 Click for large image |
Figure 2. Differential expression of PD-1 and macrophages between patients and healthy controls. Data are analyzed by Mann Whitney U-test. PD-1: programmed cell death protein 1. |
As expected, healthy controls had higher RBCs, hemoglobin (Hb) levels, WBCs, monocyte percentage, and platelet counts than patients. However, mean platelet volume (MPV) was significantly higher for healthy controls than for patients. Subsequently, MPR was comparable between both without significant differences. Moreover, NLR was significantly higher for healthy controls than for patients (Table 3).
Click to view |
Table 3. Comparison Between Patients and
Controls Regarding Hematologic Indices |
Survival analysis
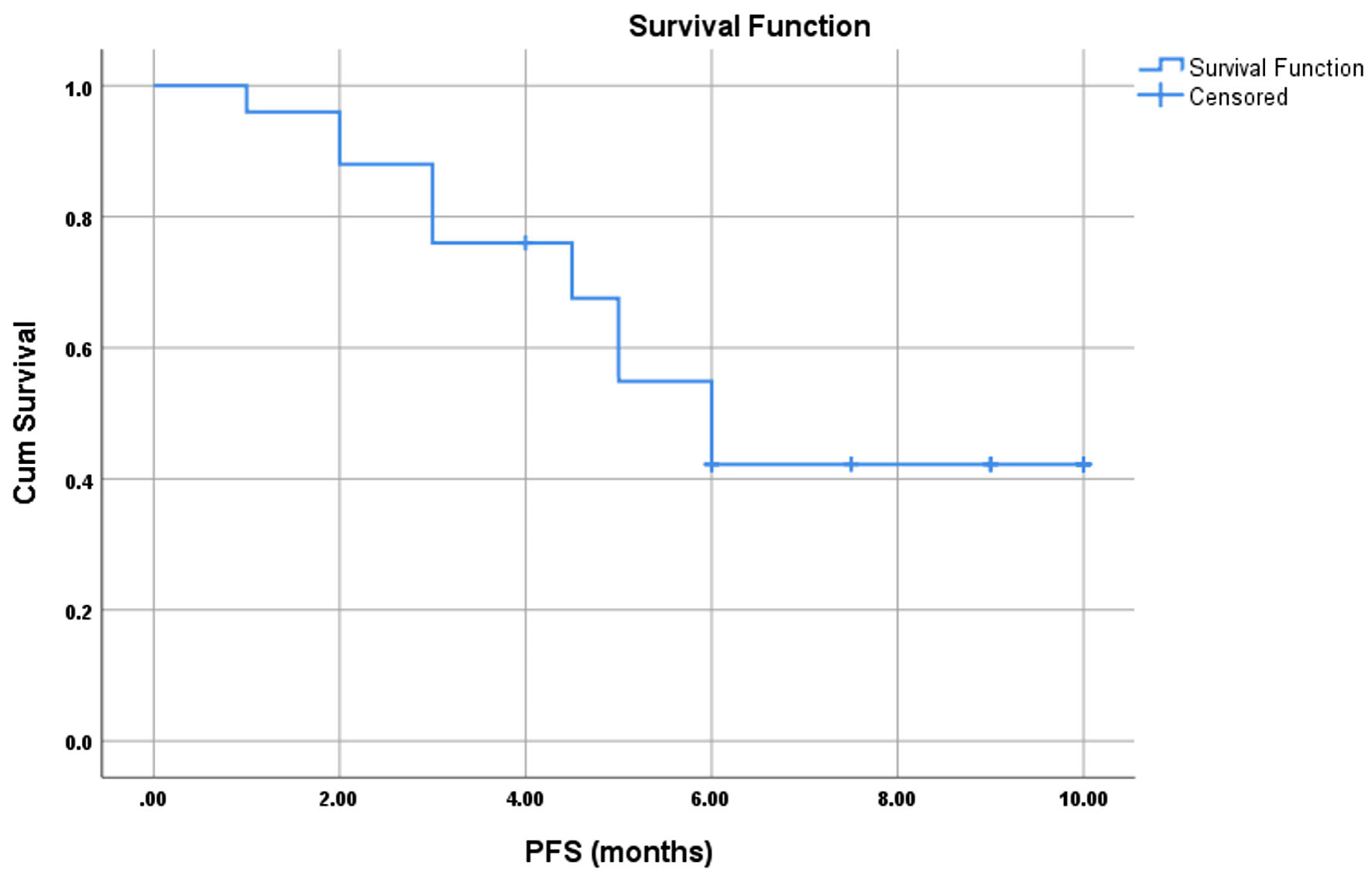
The median PFS was 6 months, and the mean ± standard error (SE) was 6.6 ± 0.64 (5.3 - 7.82) (Fig. 3). There was a significant positive correlation between PFS and CD4+ T cells and negative correlations with CD8+PD-1+ T cells and NLR. Furthermore, there were significant negative correlations between CD4+ T cells and CD4+PD-1+ and CD11b+CD68+ macrophages. Also, CD4+PD-1+ was positively correlated with CD8+PD-1+cells (Table 4).
 Click for large image |
Figure 3. PFS of 25 metastatic cholangiocarcinoma. PFS: progression-free survival |
Click to view |
Table 4. Correlations Between Survival and PD-1
Expression and Macrophages |
Relation between response type and immune cells
There was a progressive decline in CD4+ T cells with a worsening response to treatments. On the other hand, there were progressive rises in PD-1+ on either CD4+ or CD8+ T cells with worsening response. Likewise, macrophages were significantly accumulated in those with stable disease and progressive disease compared with complete response and partial response (Table 5).
Click to view |
Table 5. Disturbance of Immune Cells According
to Responses to Treatment |
Relations between immune cells and other clinicopathologic features
Only CD4+ T cells were accumulated in normal or overweight patients compared to underweight ones (mean ± standard deviation (SD) = 31.4 ± 9.7 vs. 21.7 ± 7.0, P = 0.016). In contrast, the remaining immune cells showed no significant differences between underweight and normal or overweight patients with P values of 0.3, 0.7, 0.6, 0.5, 0.3, 0.4 for CD4+PD-1+ T cells, CD8+ T cells, CD8+PD-1+ T, CD11b+CD68+ macrophages, NLR, and MPR, respectively.
Likewise, for comorbidities, we did not detect any significant association between immune cells and ratios with different comorbidities in patients even after correction for homogeneity of variances and performance of Welch test. Furthermore, no significant differences in immune cell levels according to smoking status were found except for CD4+ T cells, where they tended to be lower in currently active smokers (mean ± SD = 25.9 ± 12.1 vs. 24.1 ± 3.0 vs. 32.3 ± 7.5, P = 0.048 for the non-smoker, smoker, and ex-smoker, respectively).
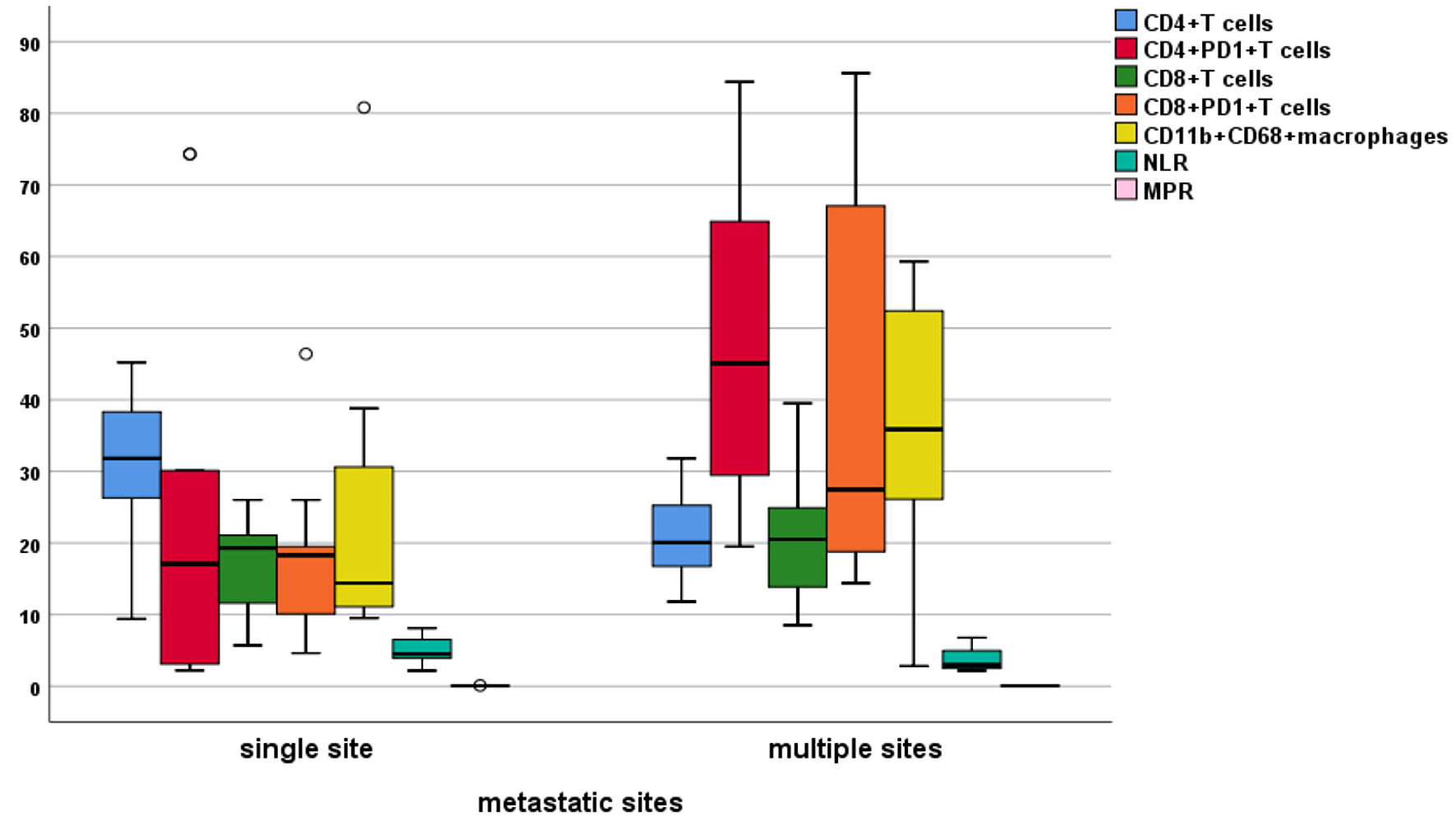
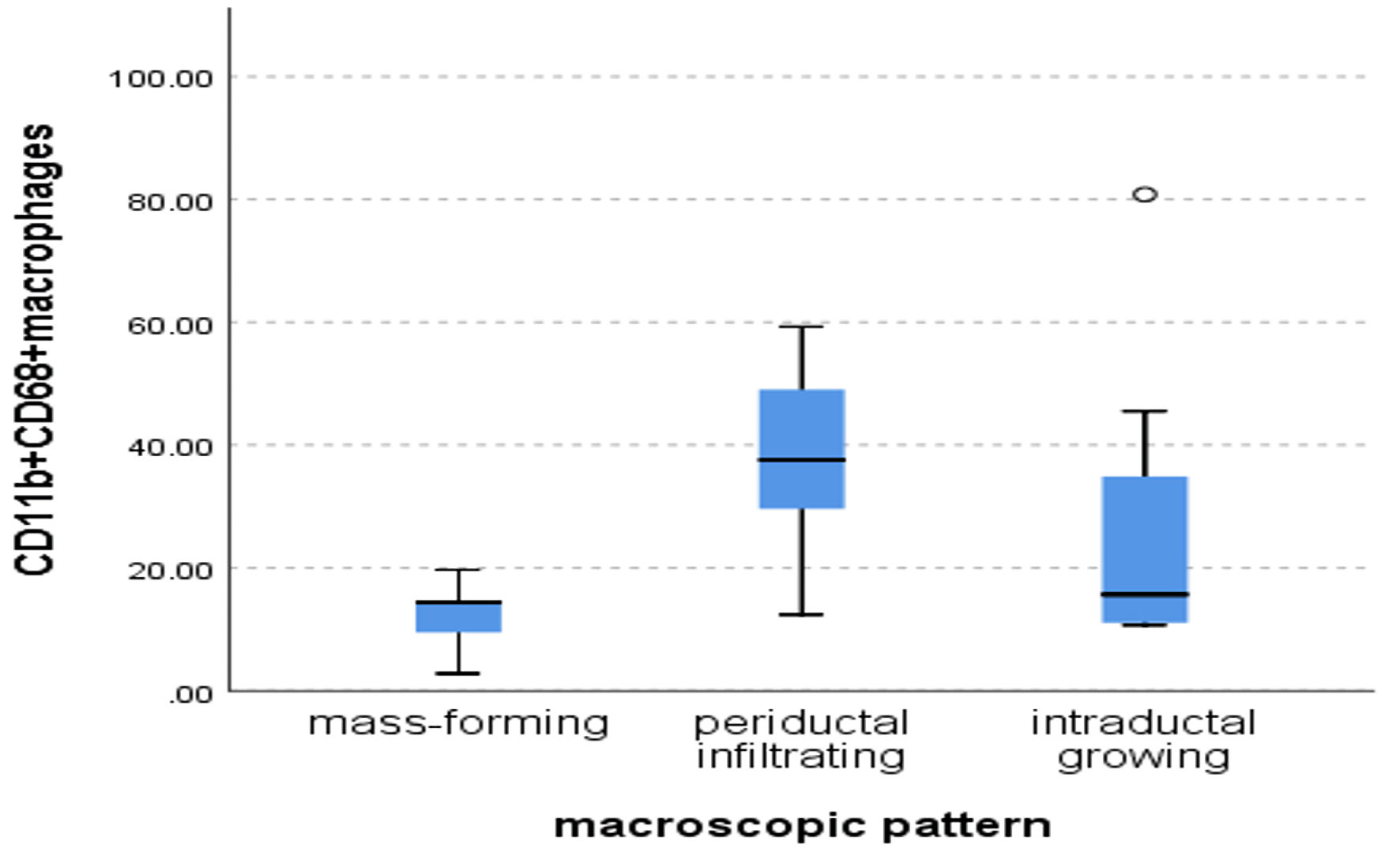
There was no significant impact of the primary site on immune cells. However, CD4+ T cells were significantly accumulated in a single site of metastasis compared to multiple organ sites (31.2 ± 9.6 vs. 21.0 ± 6.5, P = 0.012). In contrast, CD4+PD-1+ and CD8+PD-1+ T cells were significantly accumulated in patients with multiple sites of metastases compared with single sites (47.9 ± 22.9 vs. 21.7 ± 222.7, P = 0.013, and 40.8 ± 28.9 vs. 17.01 ± 10.04, P = 0.05, respectively) (Fig. 4). In addition, no significant differences in immune cells according to the macroscopic pattern were found except for macrophages, where they were accumulated in a periductal-infiltrating pattern followed by intraductal-growing then mass-forming (38.1 ± 16.9 vs. 26.7 ± 19.1 vs. 12.2 ± 6.4, respectively, P = 0.037) (Fig. 5).
 Click for large image |
Figure 4. Differential expression of immune cells between single and multiple sites of metastasis (Mann-Whitney test). PD-1: programmed cell death protein 1; NLR: neutrophil to lymphocyte ratio; MPR: mean platelet volume/platelet count ratio. |
 Click for large image |
Figure 5. Differential expression of CD11bCD68+ macrophages according to the macroscopic pattern (Kruskal Wallis test, P = 0.037). |
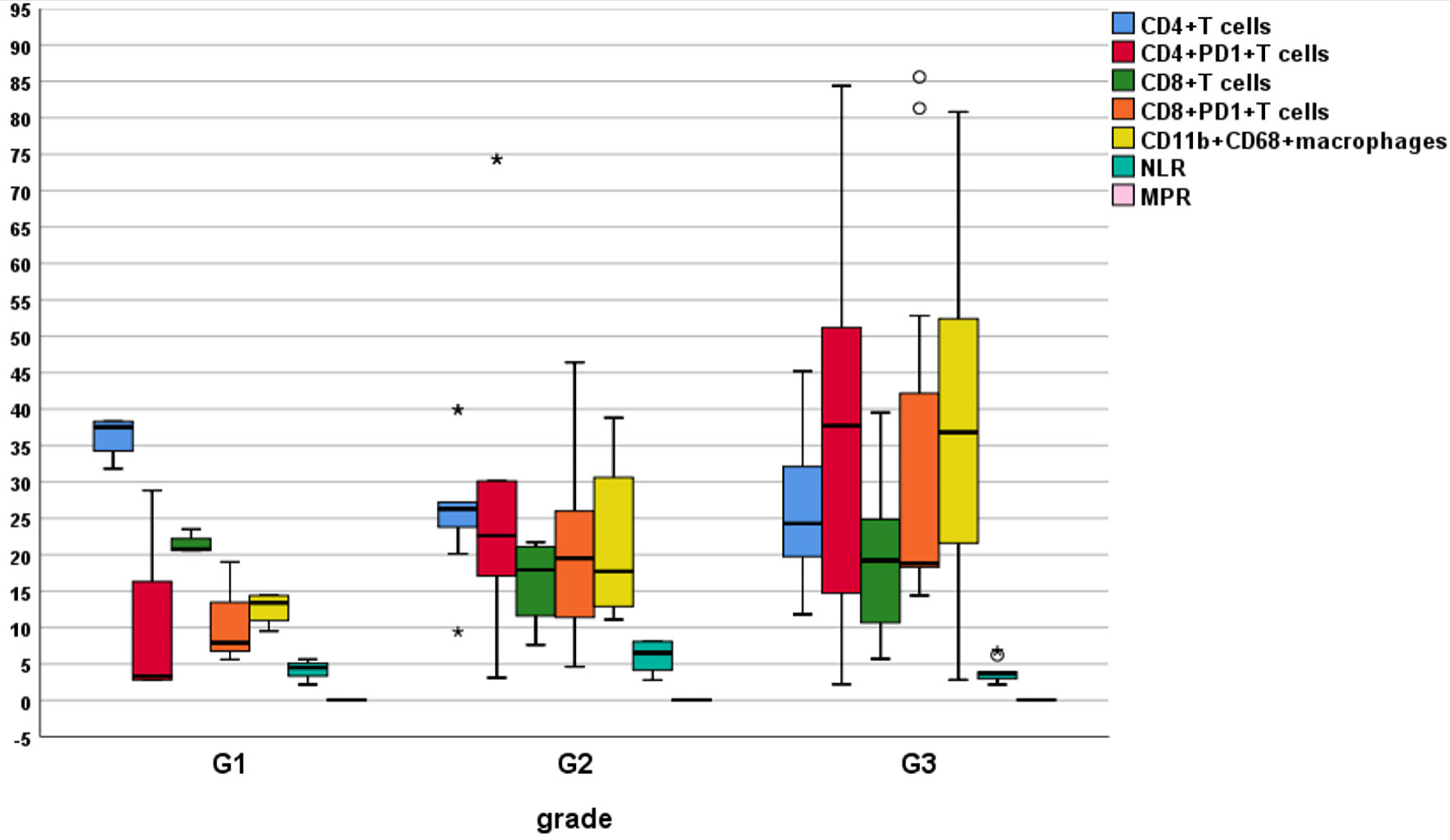
We detected a significant increase in CD4+ and CD8+ T cells in differentiated CCA, while PD-1 expression on immune cells was significantly accumulated with dedifferentiation. Likewise, CD11b+CD68+ macrophages progressively accumulated with dedifferentiation, which had a significant effect. Furthermore, as mentioned in Table 6 and Figure 6, there was no clear impact of inflammatory markers on grading.
Click to view |
Table 6. Differential Expression of Immune
Cells According to Grading |
 Click for large image |
Figure 6. Differential accumulation of immune cells according to grading. PD-1: programmed cell death protein 1; NLR: neutrophil to lymphocyte ratio; MPR: mean platelet volume/platelet count ratio. |
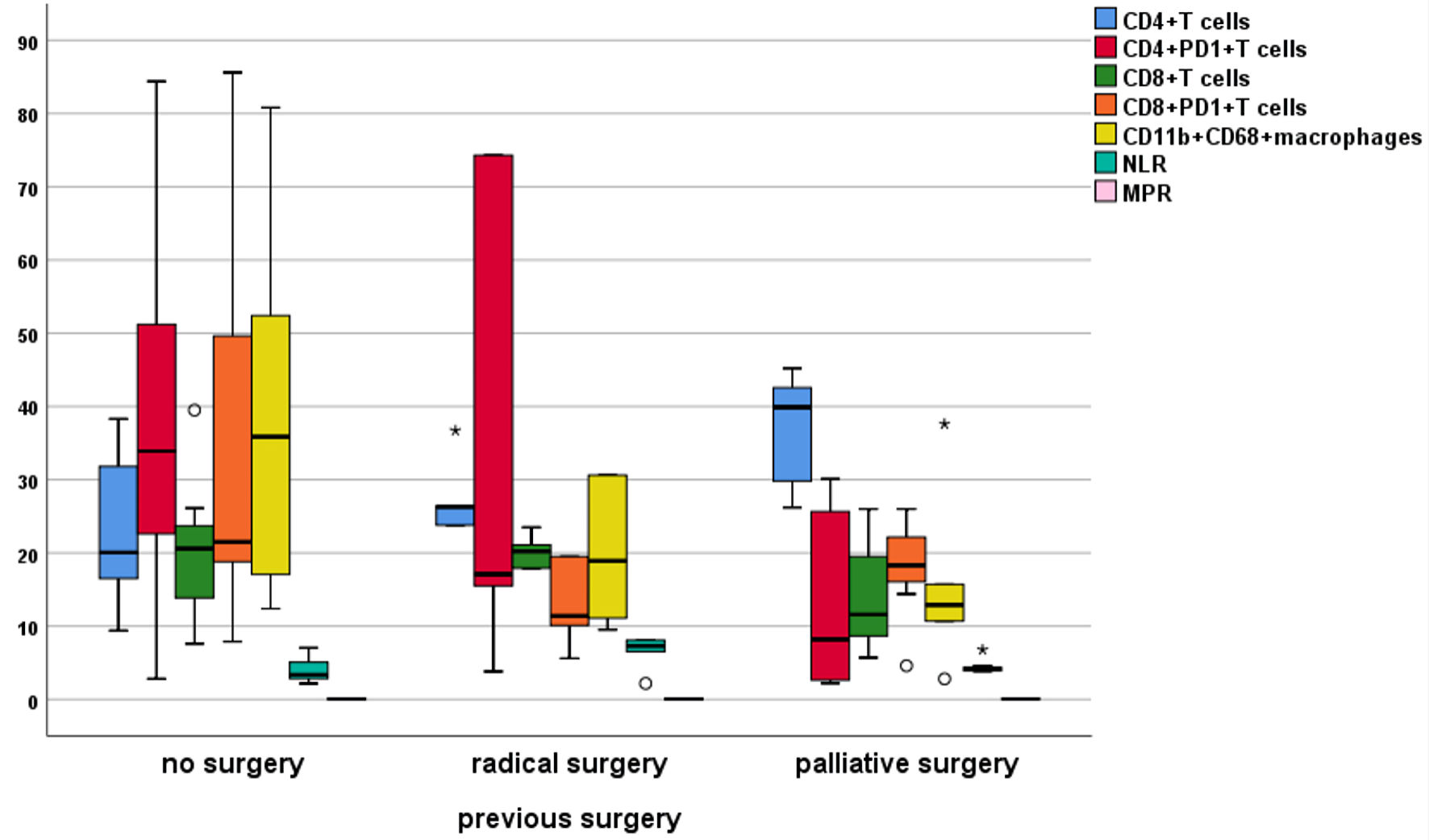
CD4+ T cells were significantly varied with the type of surgery to be accumulated, mainly in palliative surgery followed by radical surgery, compared with those without surgery. Conversely, CD8+PD-1+ cells were higher in patients without surgery compared with palliative or radical surgery. In the same manner, macrophages were significantly higher in those without surgery and progressively declined in patients with palliative and radical surgeries (Table 7, Fig. 7).
Click to view |
Table 7. Disturbances of Immune Cells According
to Previous Surgery |
 Click for large image |
Figure 7. Differential expression of immune cells according to previous surgery. PD-1: programmed cell death protein 1; NLR: neutrophil to lymphocyte ratio; MPR: mean platelet volume/platelet count ratio. |
Multivariate analysis of prognostic variables of PFS
In univariate analysis of different clinicopathological features, no significant associations between PFS and the following prognostic factors were found: age (P = 0.6), Eastern Cooperative Oncology Group performance status (ECOG-PS) (P = 0.9), comorbidities (P = 0.2), body mass index (BMI) (P = 0.2), site (P = 0.5), growth pattern (P = 0.06), and previous surgery (P = 0.4).
However, sex had a significant impact on PFS (males vs. females of 8.2 ± 4.04 vs. 5.1 ± 1.9, P = 0.03). Additionally, grades had a significant impact on PFS, with G1 at 11.3 ± 2.5, G2 at 5.4 ± 2.8, and G3 at 6.2 ± 3.3 (P = 0.009).
Moreover, patients who achieved complete response had better PFS (complete response = 8.9 ± 3.4, partial response = 5.8 ± 1.5, stable disease = 6.3 ± 3.9, and progressive disease = 3.5 ± 1.9, P = 0.042).
In multivariate analysis of significant immune cells and clinicopathologic features, the hazard of death or progression decreased three times, more than two times, and nearly two times in patients who achieved complete response, partial response, and stable disease compared to progressive disease. Furthermore, increasing NLR by one unit increased the hazard of death or progression by 0.743. The impact of immune cells was neglected because of multicollinearity with other variables like response and NLR (Table 8).
Click to view |
Table 8. Multivariate Analysis of Prognostic
Factors of PFS |
| Discussion | ▴Top |
The development of cancer is regulated by disturbed immune response and changes in homeostasis. The interaction between tumor cells and the surrounding TME successfully promotes tumor progression and metastasis. Growing evidence indicated that cellular constituents of TME, including innate cells such as macrophages, NK, dendritic cells (DCs), neutrophils, and adaptive immune cells such as T and B lymphocytes, promoted tumor spread to distant organs [19-21]. The most common source of immune cells is the peripheral blood of cancer patients, which can be assessed repeatedly to correlate the dynamic changes in their measurements with the regression or progression of tumors in response to specific therapy, particularly immunotherapy.
The current results, evaluating the role of peripheral T lymphocytes, their PD-1 expression, and peripheral macrophages in CCA outcomes and relating them to clinicopathologic characteristics, revealed higher levels of CD4+, CD8+, and CD11b+CD68+ macrophages in controls compared to patients. In contrast, PD-1 expression was significantly higher in patients compared with controls; CD4+ positively correlated with PFS, while CD8+PD-1 was negatively correlated with PFS. In general, CD4+ and CD8+ were progressively rising with improvement of response to treatments, differentiation, single organ sites, and surgical interventions. On the contrary, PD-1 expression and macrophages progressively increased with worsening of response, dedifferentiation, multiple organ sites, and surgical interventions.
Tumor cells have the ability to release different cytokines and chemokines to recruit and shape the pericellular environment to a protumor profile, A variety of cells such as fibroblasts, neutrophils, NK cells and TILs could be shaped to a protumor phenotype by CCA, among these cells are TAMs, which are derived from circulating monocytes where they deviated into protumor phenotype [22]. Progressive influx of macrophages to CCA is associated with worse CCA phenotype, recurrence, high metastatic rate, and poor prognosis [23]. It was evidenced that circulating monocytes served as a prognostic marker for CCA activity and correlated with poor pathological parameters including non-papillary type and high number of tissue macrophages [24]. In keeping with the previous studies, we explored that peripheral CD11b+CD68+ macrophages were associated with poor response to treatment, high grade CCA, periductal-infiltrating pattern, and multiple organ metastasis.
A recent report indicated that a high level of TAM in tumor-invasive front was associated with improved survival and lower recurrences in intrahepatic CCA [18]. Contrary to that report, the current results failed to detect any significant direct impact of macrophages on survival. However, indirectly, they were associated with short survival because of the high metastatic rate with multiple organ sites and disease progression.
TILs are a highly heterogeneous population derived from peripheral blood and represented mainly by CD4+, CD8+ T cells, Tregs, and B cells. These cells are responsible for adaptive immune response and are crucial for immune surveillance and tumor eradication. Previous work in intrahepatic CCA indicated that low numbers of CD4+ T cells were associated with poor survival [25]; another report showed that high levels of TILs were associated with longer survival in CCA [26]. Our results were comparable to previous studies, where the level of CD4+ T cells was significantly correlated with improved survival [25, 26].
A recent study has demonstrated that the high number of CD8+ cells in iCCA was associated with better survival, and the high level of tumor-infiltrating CD8+PD-1 was significantly correlated with advanced stage, short postoperative survival, and high-density CD68+PD-L1 [27]. Collectively, low PD-1 expression in CCA was associated with favorable outcomes, as evidenced in many studies [28-30]. The current study was in alignment with the previously mentioned ones, where CD8+PD-1 was correlated with poor PFS. In addition, PD-1 expression was associated with disease progression, inadequate response and poor clinicopathologic characteristics.
An embarrassing recent work in pCCA reported that high CD8+PD-1 levels were associated with improved median survival and recurrence-free survival and considered them an independent predictor for better survival in multivariate analysis (hazard ratio (HR) = 0.42, P = 0.031), which was explained by high nerve fiber density detected in these tumors [31], and therefore indicated that the prognostic relevance of PD-1 is diverse. The expression of this marker and its ligands by themselves are not sufficient for prognosis without taking into consideration other immune cells in TME.
Furthermore, the pertinence of NLR to immune cells and survival was indefinite in the current study, where it was not related to immune cell levels, PD-1+ expression, response to chemotherapy, grading, primary tumor sites and macroscopic patterns, and site of metastasis, but it was correlated with short PFS (r = -0.5, P = 0.015), and its level was progressively rising from those without surgical intervention to radical surgery (P = 0.016). These results were hardly aligned with those of Lin et al, where NLR was correlated with PD-1+ expression and also related to short survival [32].
The standard treatment for advanced CCA is the gemcitabine-cisplatin regimen, which modestly increased the median survival compared with gemcitabine alone. Also, the addition of nab-paclitaxel to this regimen further prolonged PFS (11.8 months) and median survival (19.2 months). Other regimens including gemcitabine and fluoropyrimidine were approved, but in general chemotherapeutic regimens had limited efficacy in CCA. To improve therapeutic outcomes, targeting of TME was studied in several reports focusing on targeting of PD-1, cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), and TAMs. Pembrolizumab (monoclonal anti-PD-1 antibody) was associated with 100% disease control rate (DCR) in CCA with high microsatellite instability (MSI-H)/deficient mismatch repair (dMMR). Also, in the analysis of pembrolizumab in five uncontrolled single-arm studies, including 149 patients with MSI-H/MMR-deficient tumors (KEYNOTE-012, 016, 028, 158, 164) (90 metastatic colorectal cancers and 59 other tumor types, including 11 biliary tract cancers), the objective response rate (ORR) was 39.6% and persisted for ≥ 6 months in 78% of them; moreover 27% of CCA patients had a duration of response ranged from 11.6 to 19.6 months [33].
A recent meta-analysis [34] involved all phase II and III trials to compare immunotherapy protocols in patients with solid malignancies. The pooled results showed that immunotherapy was associated with improved PFS in patients with good PS (ECOG-PS: 0 - 1). In the current results, PFS was not improved in patients with PS = 0, compared to PS = 1 - 2. Furthermore, no immunotherapy was given despite being the preferred treatment in combination with chemotherapy for CCA.
We focused on the peripheral blood mononuclear cells (PBMCs) because they were easier to obtain than tissue biopsies and more convenient for clinical applications. Furthermore, we found that the immune landscape of the PBMCs in CCA patients before treatment could reflect the state of systemic immune function and response to treatments; and importantly, it can be used to identify biological markers to predict the response of chemotherapy.
Limitations of the study
The study has several limitations. It was carried out on metastatic cases, and better work needs to be done on different stages of CCA to define the role of immune cells properly. Also, macrophages and PD-1 should be evaluated on TME in addition to peripheral blood. The current results need to be validated in a larger sample size and sub-grouped according to operability. Furthermore, a national and international collaboration between cancer centers is required.
Conclusions
CCA has a desmoplastic microenvironment with complex immunologic topography and tumor-reactive stroma. The immune landscape of the PBMCs in CCA patients before treatment could reflect the state of systemic immune function and response to treatments. Our results revealed that T lymphocytes correlated with better prognosis while macrophages and PD-1+ expression were associated with poor outcomes.
Acknowledgments
The authors acknowledge the Assiut University for support.
Financial Disclosure
None to declare.
Conflict of Interest
All authors declared that they had no conflict of interest.
Informed Consent
Informed written consent was obtained from all cases and controls.
Author Contributions
AMZ, AR, KS, KR, AS, DAG, EEMOM and MAR contributed to the study’s design, patient follow-up, and data analysis. AMZ, HME, ZAMZ and AR conducted all investigations for the study. AKI, MMF, and KS prepared the manuscript draft. All authors participated in the critical review of the final manuscript version, approved the manuscript in its submitted form, and agreed to take responsibility for all aspects of the work.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Blechacz B. Cholangiocarcinoma: current knowledge and new
developments. Gut Liver. 2017;11(1):13-26.
doi pubmed pmc - Rizzo A, Brandi G. Pitfalls, challenges, and updates in
adjuvant systemic treatment for resected biliary tract cancer. Expert Rev Gastroenterol Hepatol.
2021;15(5):547-554.
doi pubmed - Banales JM, Marin JJG, Lamarca A, Rodrigues PM, Khan SA,
Roberts LR, Cardinale V, et al. Cholangiocarcinoma 2020: the next horizon in mechanisms and
management. Nat Rev Gastroenterol Hepatol. 2020;17(9):557-588.
doi pubmed pmc - Rizzo A, Mollica V, Tateo V, Tassinari E, Marchetti A,
Rosellini M, De Luca R, et al. Hypertransaminasemia in cancer patients receiving immunotherapy
and immune-based combinations: the MOUSEION-05 study. Cancer Immunol Immunother.
2023;72(6):1381-1394.
doi pubmed pmc - Ezzat R, Eltabbakh M, El Kassas M. Unique situation of
hepatocellular carcinoma in Egypt: A review of epidemiology and control measures.
World J Gastrointest Oncol. 2021;13(12):1919-1938.
doi pubmed pmc - Rizzo A, Brandi G. Neoadjuvant therapy for
cholangiocarcinoma: A comprehensive literature review. Cancer Treat Res Commun.
2021;27:100354.
doi pubmed - Fabris L, Perugorria MJ, Mertens J, Bjorkstrom NK, Cramer T,
Lleo A, Solinas A, et al. The tumour microenvironment and immune milieu of cholangiocarcinoma.
Liver Int. 2019;39(Suppl 1):63-78.
doi pubmed pmc - Xu F, Jin T, Zhu Y, Dai C. Immune checkpoint therapy in
liver cancer. J Exp Clin Cancer Res. 2018;37(1):110.
doi pubmed pmc - Ziani L, Chouaib S, Thiery J. Alteration of the antitumor
immune response by cancer-associated fibroblasts. Front Immunol. 2018;9:414.
doi pubmed pmc - Dwyer BJ, Jarman EJ, Gogoi-Tiwari J, Ferreira-Gonzalez S,
Boulter L, Guest RV, Kendall TJ, et al. TWEAK/Fn14 signalling promotes cholangiocarcinoma niche
formation and progression. J Hepatol. 2021;74(4):860-872.
doi pubmed - Subimerb C, Pinlaor S, Khuntikeo N, Leelayuwat C, Morris A,
McGrath MS, Wongkham S. Tissue invasive macrophage density is correlated with prognosis in
cholangiocarcinoma. Mol Med Rep. 2010;3(4):597-605.
doi pubmed - Raggi C, Correnti M, Sica A, Andersen JB, Cardinale V,
Alvaro D, Chiorino G, et al. Cholangiocarcinoma stem-like subset shapes tumor-initiating niche
by educating associated macrophages. J Hepatol. 2017;66(1):102-115.
doi pubmed pmc - Wu HJ, Chu PY. Role of cancer stem cells in
cholangiocarcinoma and therapeutic implications. Int J Mol Sci. 2019;20(17):4154.
doi pubmed pmc - Fabris L, Cadamuro M, Cagnin S, Strazzabosco M, Gores GJ.
Liver matrix in benign and malignant biliary tract disease. Semin Liver Dis.
2020;40(3):282-297.
doi pubmed - Ahmadzadeh M, Johnson LA, Heemskerk B, Wunderlich JR, Dudley
ME, White DE, Rosenberg SA. Tumor antigen-specific CD8 T cells infiltrating the tumor express
high levels of PD-1 and are functionally impaired. Blood. 2009;114(8):1537-1544.
doi pubmed pmc - Staron MM, Gray SM, Marshall HD, Parish IA, Chen JH, Perry
CJ, Cui G, et al. The transcription factor FoxO1 sustains expression of the inhibitory receptor
PD-1 and survival of antiviral CD8(+) T cells during chronic infection. Immunity.
2014;41(5):802-814.
doi pubmed pmc - Messenheimer DJ, Jensen SM, Afentoulis ME, Wegmann KW, Feng
Z, Friedman DJ, Gough MJ, et al. Timing of PD-1 blockade is critical to effective combination
immunotherapy with anti-OX40. Clin Cancer Res. 2017;23(20):6165-6177.
doi pubmed pmc - Atanasov G, Dietel C, Feldbrugge L, Benzing C, Krenzien F,
Brandl A, Mann E, et al. Tumor necrosis and infiltrating macrophages predict survival after
curative resection for cholangiocarcinoma. Oncoimmunology. 2017;6(8):e1331806.
doi pubmed pmc - Sceneay J, Griessinger CM, Hoffmann SHL, Wen SW, Wong CSF,
Krumeich S, Kneilling M, et al. Tracking the fate of adoptively transferred myeloid-derived
suppressor cells in the primary breast tumor microenvironment. PLoS One.
2018;13(4):e0196040.
doi pubmed pmc - Tomas-Bort E, Kieler M, Sharma S, Candido JB, Loessner D. 3D
approaches to model the tumor microenvironment of pancreatic cancer. Theranostics.
2020;10(11):5074-5089.
doi pubmed pmc - Hinshaw DC, Shevde LA. The Tumor Microenvironment Innately
Modulates Cancer Progression. Cancer Res. 2019;79(18):4557-4566.
doi pubmed pmc - Zhou M, Wang C, Lu S, Xu Y, Li Z, Jiang H, Ma Y.
Tumor-associated macrophages in cholangiocarcinoma: complex interplay and potential therapeutic
target. EBioMedicine. 2021;67:103375.
doi pubmed pmc - Sun D, Luo T, Dong P, Zhang N, Chen J, Zhang S, Liu L, et
al. CD86(+)/CD206(+) tumor-associated macrophages predict prognosis of patients with
intrahepatic cholangiocarcinoma. PeerJ. 2020;8:e8458.
doi pubmed pmc - Subimerb C, Pinlaor S, Lulitanond V, Khuntikeo N, Okada S,
McGrath MS, Wongkham S. Circulating CD14(+) CD16(+) monocyte levels predict tissue invasive
character of cholangiocarcinoma. Clin Exp Immunol. 2010;161(3):471-479.
doi pubmed pmc - Carapeto F, Bozorgui B, Shroff RT, Chagani S, Solis Soto L,
Foo WC, Wistuba I, et al. The immunogenomic landscape of resected intrahepatic
cholangiocarcinoma. Hepatology. 2022;75(2):297-308.
doi pubmed pmc - Goeppert B, Frauenschuh L, Zucknick M, Stenzinger A,
Andrulis M, Klauschen F, Joehrens K, et al. Prognostic impact of tumour-infiltrating immune
cells on biliary tract cancer. Br J Cancer. 2013;109(10):2665-2674.
doi pubmed pmc - Tian L, Ma J, Ma L, Zheng B, Liu L, Song D, Wang Y, et al.
PD-1/PD-L1 expression profiles within intrahepatic cholangiocarcinoma predict clinical outcome.
World J Surg Oncol. 2020;18(1):303.
doi pubmed pmc - Lu JC, Zeng HY, Sun QM, Meng QN, Huang XY, Zhang PF, Yang X,
et al. Distinct PD-L1/PD1 Profiles and Clinical Implications in Intrahepatic Cholangiocarcinoma
Patients with Different Risk Factors. Theranostics. 2019;9(16):4678-4687.
doi pubmed pmc - Kitano Y, Yamashita YI, Nakao Y, Itoyama R, Yusa T, Umezaki
N, Tsukamoto M, et al. Clinical Significance of PD-L1 Expression in Both Cancer and Stroma Cells
of Cholangiocarcinoma Patients. Ann Surg Oncol. 2020;27(2):599-607.
doi pubmed - Gani F, Nagarajan N, Kim Y, Zhu Q, Luan L, Bhaijjee F,
Anders RA, et al. Program Death 1 Immune Checkpoint and Tumor Microenvironment: Implications for
Patients With Intrahepatic Cholangiocarcinoma. Ann Surg Oncol. 2016;23(8):2610-2617.
doi pubmed - Tan X, Bednarsch J, Rosin M, Appinger S, Liu D, Wiltberger
G, Garcia Vallejo J, et al. PD-1+ T-cells correlate with nerve fiber density as a prognostic
biomarker in patients with resected perihilar cholangiocarcinoma. Cancers (Basel).
2022;14(9):2190.
doi pubmed pmc - Lin G, Liu Y, Li S, Mao Y, Wang J, Shuang Z, Chen J, et al.
Elevated neutrophil-to-lymphocyte ratio is an independent poor prognostic factor in patients
with intrahepatic cholangiocarcinoma. Oncotarget. 2016;7(32):50963-50971.
doi pubmed pmc - Loeuillard E, Conboy CB, Gores GJ, Rizvi S. Immunobiology of
cholangiocarcinoma. JHEP Rep. 2019;1(4):297-311.
doi pubmed pmc - Mollica V, Rizzo A, Marchetti A, Tateo V, Tassinari E,
Rosellini M, Massafra R, et al. The impact of ECOG performance status on efficacy of
immunotherapy and immune-based combinations in cancer patients: the MOUSEION-06 study. Clin Exp
Med. 2023;23(8):5039-5049.
doi pubmed
This
article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0
International License, which permits unrestricted non-commercial use, distribution, and
reproduction in any medium, provided the original work is properly cited.
Journal
of Clinical Medicine Research is published by Elmer Press Inc.