


Effectiveness of Antibiotic Regimens in Reducing White Blood Cell Count Within Three to Five Days in Febrile Leukocytosis Treated With Ambulatory Therapy
DOI:
https://doi.org/10.14740/jocmr6339Keywords:
Fever, Leukocytosis, Anti-bacterial agents, Ambulatory care, Treatment outcome, Leukocyte countAbstract
Background: In the absence of sepsis, patients with fever and leukocytosis in the emergency department (ED) are often treated with ambulatory parenteral antibiotics at the physician’s discretion. Identifying effective regimens for reducing white blood cell (WBC) count and improving clinical outcomes may support standardized ED care.
Methods: This retrospective cohort included adult ED patients with fever and leukocytosis, but without sepsis, in whom basic investigation revealed no clear source of infection. Patients received one of three regimens: (A) single-day intravenous (IV) ceftriaxone followed by oral cefixime, (B) 3-day IV ceftriaxone followed by oral cefixime, or (C) 3-day IV ceftriaxone plus oral doxycycline from day 1. Demographics, baseline data, and laboratory results were collected. Follow-up assessments included WBC count and clinical improvement. Treatment probabilities were estimated with multinomial logistic regression, and stabilized inverse probability of treatment weighting (IPTW) were applied in weighted quantile regression.
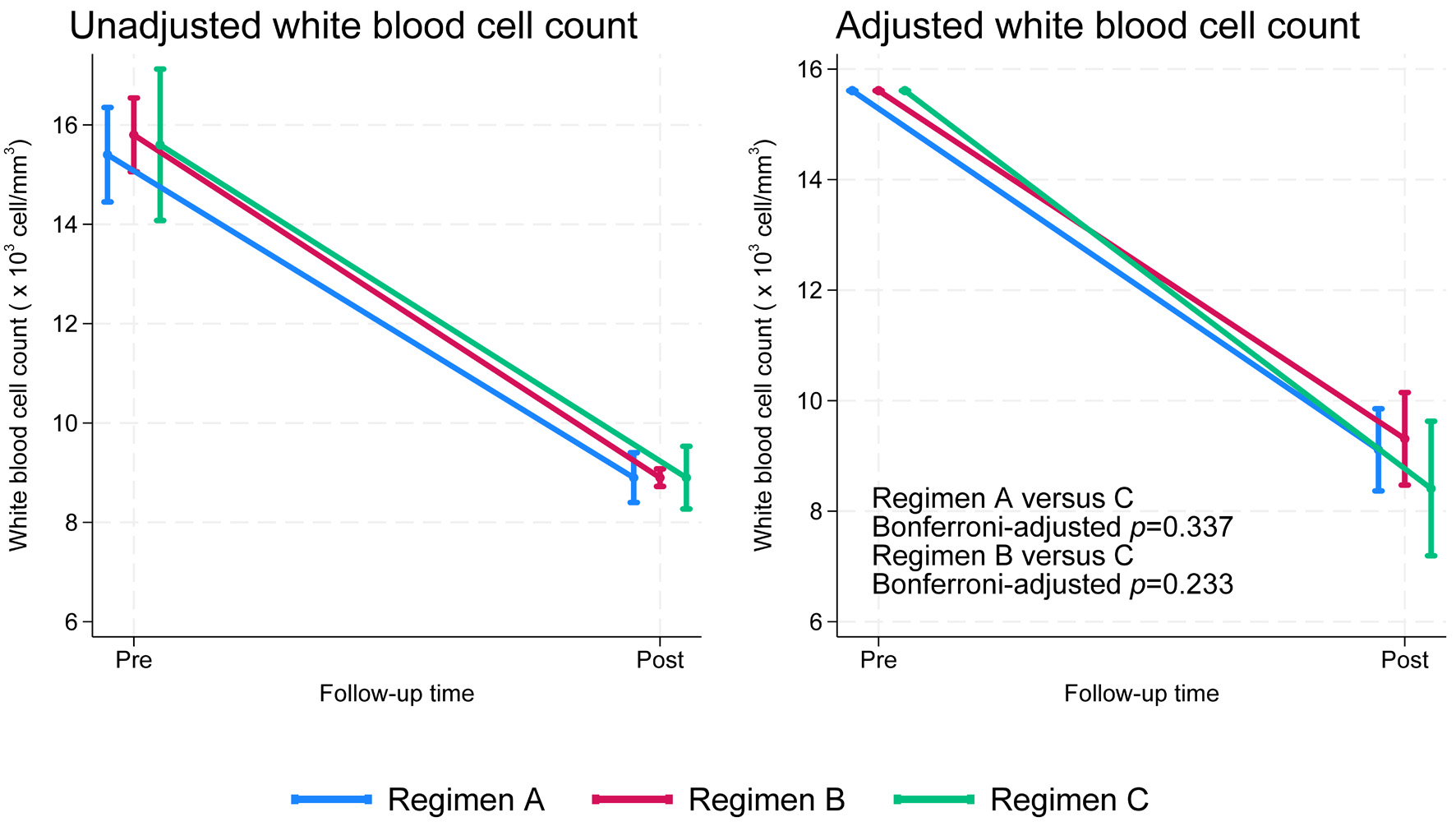
Results: Among 250 patients, most were female (63.2%) with a mean age of 49 years. After adjustment, regimen C showed a median WBC reduction of -6.9 × 103 cells/mm3 (95% confidence interval (CI): -7.5 to -6.3), compared with -6.8 × 103 (95% CI: -7.2 to -6.5) for regimen B and -6.6 × 103 (95% CI: -7.0 to -6.2) for regimen A. Differences were not significant (Wald test, P = 0.484), but graphical analysis suggested the steepest decline with regimen C.
Conclusion: Though regimen C showed the steepest WBC decline and fewer failures, the study was markedly underpowered (< 10%). Larger multicenter studies are required to confirm these findings.
Published
Issue
Section
License
Copyright (c) 2025 The authors

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.





