


Improving a Clinical Prediction Model for Computed Tomography Head Scan Use in Non-Traumatic Seizures: The SeizCT Optimized Model
DOI:
https://doi.org/10.14740/jocmr6282Keywords:
Seizures, Computed tomography, Glasgow Coma Scale, Clinical prediction rules, Diagnosis, Mobile applicationsAbstract
Background: A previous study developed a predictive model for identifying positive findings on computed tomography (CT) brain imaging in patients with non-traumatic seizures. One key predictor was the Glasgow Coma Scale (GCS), categorized into three groups (≤ 8, 9 - 13, >13). However, in real-world practice, some bedridden patients have low baseline GCS, which may lead to overprediction and unnecessary CT imaging. The original model yielded a false positive of 16.6%, exceeding the predefined threshold of less than 15%. This study aimed to improve the model by replacing categorized GCS with GCS change from baseline to reduce false positives below 15%, while maintaining false negatives below 5%.
Methods: This diagnostic predictive study included patients with non-traumatic seizures who underwent CT brain imaging at the emergency department between November 2019 and November 2023. The original predictors were retained, with GCS change from baseline replacing the categorized GCS. Multivariable logistic regression analysis was used to estimate multivariable odds ratios. Discriminative performance was assessed using the area under the receiver operating characteristic (AuROC) curve. A trade-off between sensitivity and specificity was applied to identify a probability cut-off that met the target for false positives and false negatives. The revised model was named the “SeizCT optimized model”.
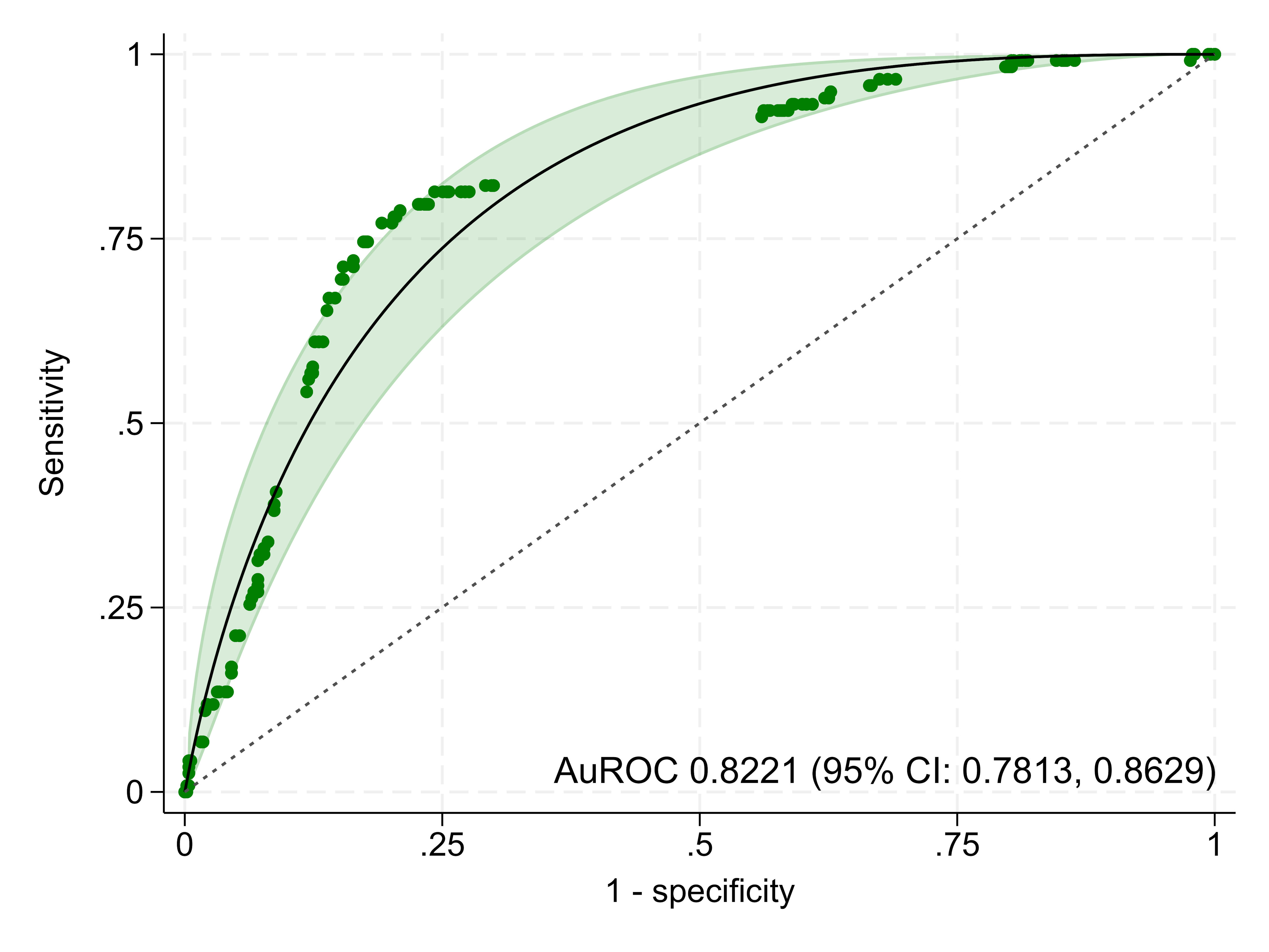
Results: Of the 625 patients included, 18.9% had positive CT findings. The majority were male (74.9%) with a mean age of 55 years. The SeizCT optimized model incorporated six predictors: prior stroke (> 3 months), current cancer, GCS change from baseline, alcohol withdrawal symptoms, epilepsy, and focal neurological deficit. The model demonstrated an AuROC of 0.8221 (95% confidence interval (CI): 0.7813, 0.8629). Using a threshold probability of 22.57%, it outperformed the original model (AuROC of 0.8156; 95% CI: 0.7598, 0.8746) with narrower confidence intervals. It achieved a false negative of 4.8% and a false positive of 14.4%.
Conclusions: The SeizCT optimized model showed improved performance over the original tool, reducing both false positives and false negatives within the predefined thresholds. External validation is recommended.
Published
Issue
Section
License
Copyright (c) 2025 The authors

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.





