


Bilateral Adrenalectomy for Primary Bilateral Macronodular Adrenocortical Hyperplasia With a Novel ARMC5 Mutation Site
DOI:
https://doi.org/10.14740/jocmr6359Keywords:
Primary bilateral macronodular adrenocortical hyperplasia, ARMC5, Adrenal venous sampling, Cushing syndromeAbstract
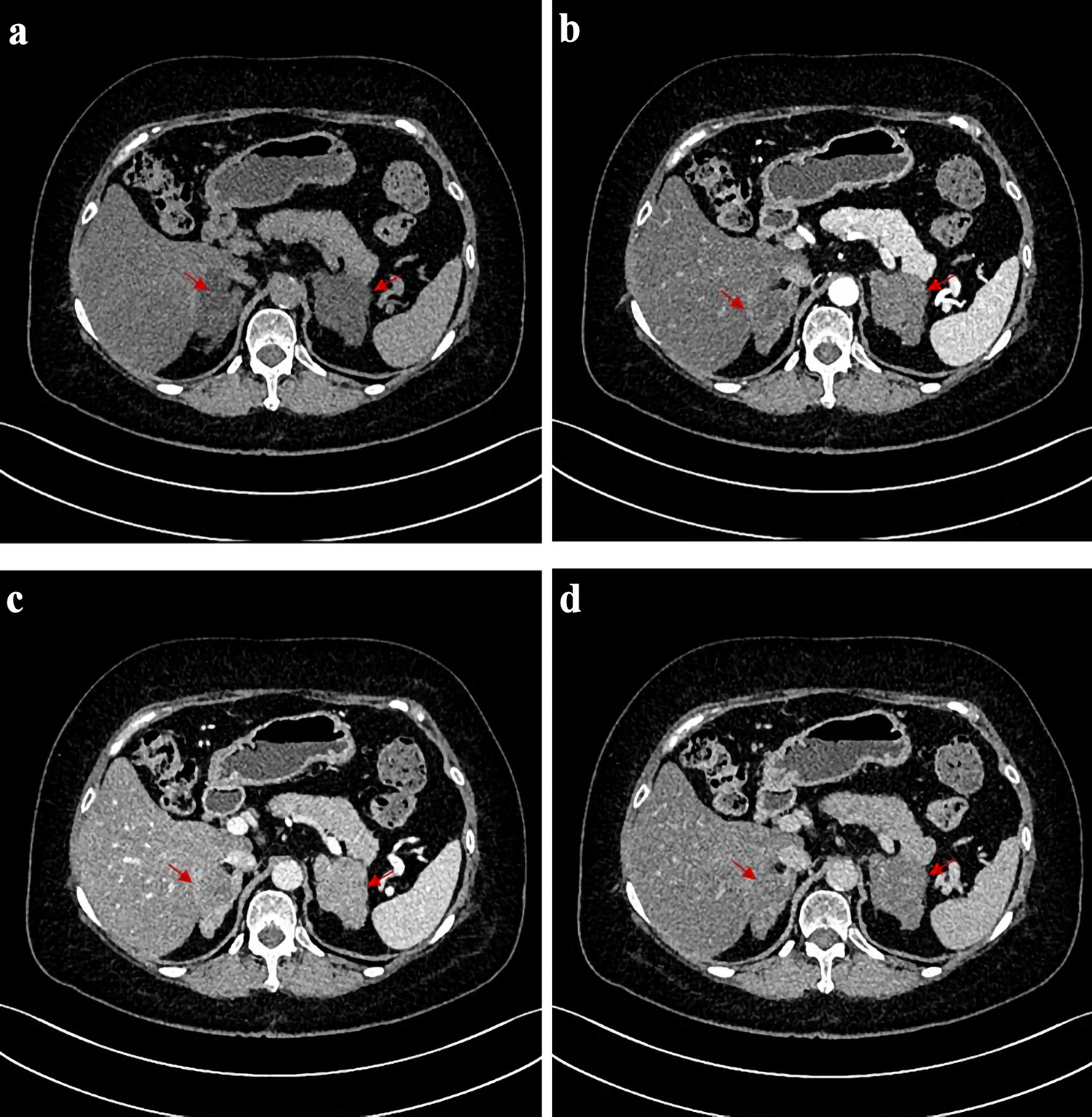
Primary bilateral macronodular adrenocortical hyperplasia (PBMAH) is a heterogeneous disorder, with clinical spectrum ranging from subclinical to severe overt Cushing syndrome (CS). Armadillo repeat containing 5 (ARMC5) mutations, found in 20-55% of cases, are often associated with more severe disease, and specific genotypes may correlate with distinct phenotypes. A 60-year-old woman was admitted with a 1-year history of progressive weight gain and hypokalemia, alongside a 13-year history of refractory hypertension. She exhibited classic CS features and metabolic complications, including hypertension and diabetes. Laboratory tests revealed elevated cortisol, suppressed adrenocorticotropic hormone (ACTH), and positive low- and high-dose dexamethasone suppression tests. Contrast-enhanced computed tomography (CT) showed bilateral irregular macronodular adrenal masses. Adrenal venous sampling (AVS) demonstrated no lateralization (lateralization index < 4). Whole-exome sequencing of peripheral blood leukocytes identified a novel ARMC5 mutation (c.534_555dup, p.Ser186Profs*19). A right adrenalectomy was performed in 2023. Although symptoms improved, cortisol levels remained significantly elevated. Consequently, a left adrenalectomy was performed 15 months later in 2024, which led to marked improvement in her CS symptoms, biomarker levels, and metabolic complications. This case report describes a novel ARMC5 mutation site in a PBMAH patient who ultimately required bilateral adrenalectomy. While AVS combined with CT can help determine the dominant side for surgery, patients with ARMC5 mutations and symmetrically sized tumors often require bilateral adrenalectomy for cure.
Published
Issue
Section
License
Copyright (c) 2025 The authors

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.





