


PIFA-N Multifactor Model to Predict Adverse Outcomes for Chronic Heart Failure Patients
DOI:
https://doi.org/10.14740/jocmr6518Keywords:
Chronic heart failure, Multifactor prognostic model, Prognostic factors, NT-proBNPAbstract
Background: In recent years, special attention has been given to developing multifactor models that support a more personal approach to assessing prognosis for chronic heart failure (CHF) patients with varying degrees of systolic dysfunction. The existing scales, namely the Seattle Heart Failure Model (SHFM), Meta-Analysis Global Group in Chronic HF (MAGGIC-HF), PARADIGM Risk of Events and Death in the Contemporary Treatment (PREDICT-HF), and the Barcelona Bio-HF (BCN-Bio-HF) risk calculator, contain numerous variables and biomarkers not readily accessible in actual clinical practice and thus fall short of meeting physicians’ requirements. The study aimed to develop a multifactor model for assessing the risk of comorbid CHF patients developing adverse outcomes.
Methods: Our study included 233 patients (129 male and 104 female) aged 73.2 ± 12.4 years, admitted to the Internal Medicine Clinic of the Sechenov University Clinical Hospital No. 4 with symptoms of New York Heart Association Functional Classification (NYHA FC) II to IV CHF, including 91 patients with heart failure with preserved ejection fraction (CHFpEF), 69 with heart failure with mildly reduced ejection fraction (CHFmrEF), and 63 with heart failure with reduced ejection fraction (CHFrEF). All the patients had given their informed and written consent to take part in the study. They were given a standard clinical examination and additionally tested for N-terminal pro-B-type natriuretic peptide (NT-proBNP), soluble interleukin-like protein receptor (sST2), galectin-3, hepcidin, and copeptin levels. Prospective follow-up lasted for 36 ± 3 months. The primary endpoint was defined as death from all causes. The findings were processed statistically using Statistica 12.0 and SPSS software.
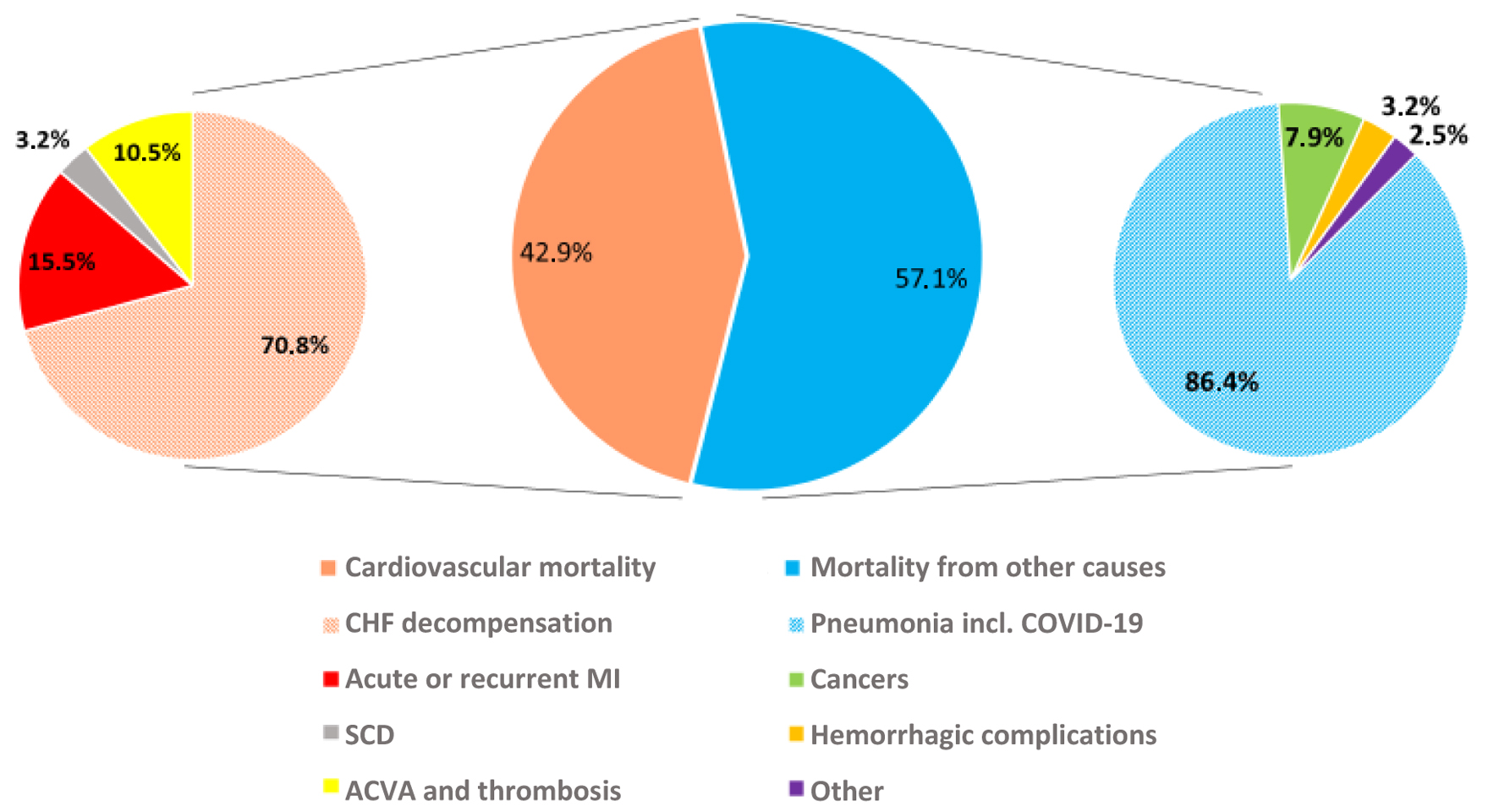
Results: All-cause mortality was 33.1% in the cohort examined. We used uni- and multivariate regression analysis to develop a PIFA-N prognostic mathematical model of adverse outcome that factored in community-acquired pneumonia diagnosed on inclusion in the study (odds ratio (OR): 3.09, 95% confidence interval (CI) 1.13–8.5, P = 0.028), a previous myocardial infarction (OR: 4.26, 95% CI 1.54–11.7, P = 0.005), presence of any form of atrial fibrillation (OR: 3.13, 95% CI 1.05–9.2, P = 0.039) and/or anemia (OR: 3.18, 95% CI 1.003–10.1, P = 0.049), and NT-proBNP level (OR: 1.0005, 95% CI 1.0002–1.0008, P = 0.002). Other biomarkers studied showed no predictive value. Our PIFA-N model is 77.1% sensitive and 77.3% specific (area under receiver operating characteristic curve (ROC AUC) 0.845), which meets high efficiency criteria.
Conclusion: We analyzed CHF patients’ 3-year survival rate to develop an efficient prognostic model for assessing the risk of lethal outcome, whose arguments are easy-to-check conditions and routine laboratory test figures that can be established without any sophisticated examination techniques.
Published
Issue
Section
License
Copyright (c) 2026 The authors

This work is licensed under a Creative Commons Attribution 4.0 International License.





