


Baseline Lactate Dehydrogenase Predicts Early Treatment Failure in Diffuse Large B-Cell Lymphoma Treated With R-CHOP: A Real-World Cohort Study
DOI:
https://doi.org/10.14740/jocmr6583Keywords:
Diffuse large B-cell lymphoma, Early treatment failure, Primary refractory, Early relapse, Lactate dehydrogenase, R-CHOPAbstract
Background: Early treatment failure following first-line R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) remains a major clinical problem in diffuse large B-cell lymphoma (DLBCL), particularly in real-world settings where late presentation and variable access to diagnostics may shape outcomes. We examined clinical and laboratory predictors of time-to-diagnosis associated with early treatment failure in an Indonesian referral-center cohort.
Methods: We performed a retrospective observational cohort study at Dharmais National Cancer Center Hospital, Jakarta, including adults with DLBCL who initiated first-line R-CHOP between January 2019 and June 2024 and had evaluable baseline data and response assessment. Early treatment failure was defined as primary refractory disease (stable/progressive disease during or at the end of treatment, or a partial response at the end of treatment) or early recurrence occurring within ≤ 12 months following the attainment of complete response. Candidate predictors were analyzed using logistic regression; a prespecified multivariable model included age > 60 years, Eastern Cooperative Oncology Group (ECOG) performance status, Ann Arbor stage, anemia, and lactate dehydrogenase (LDH).
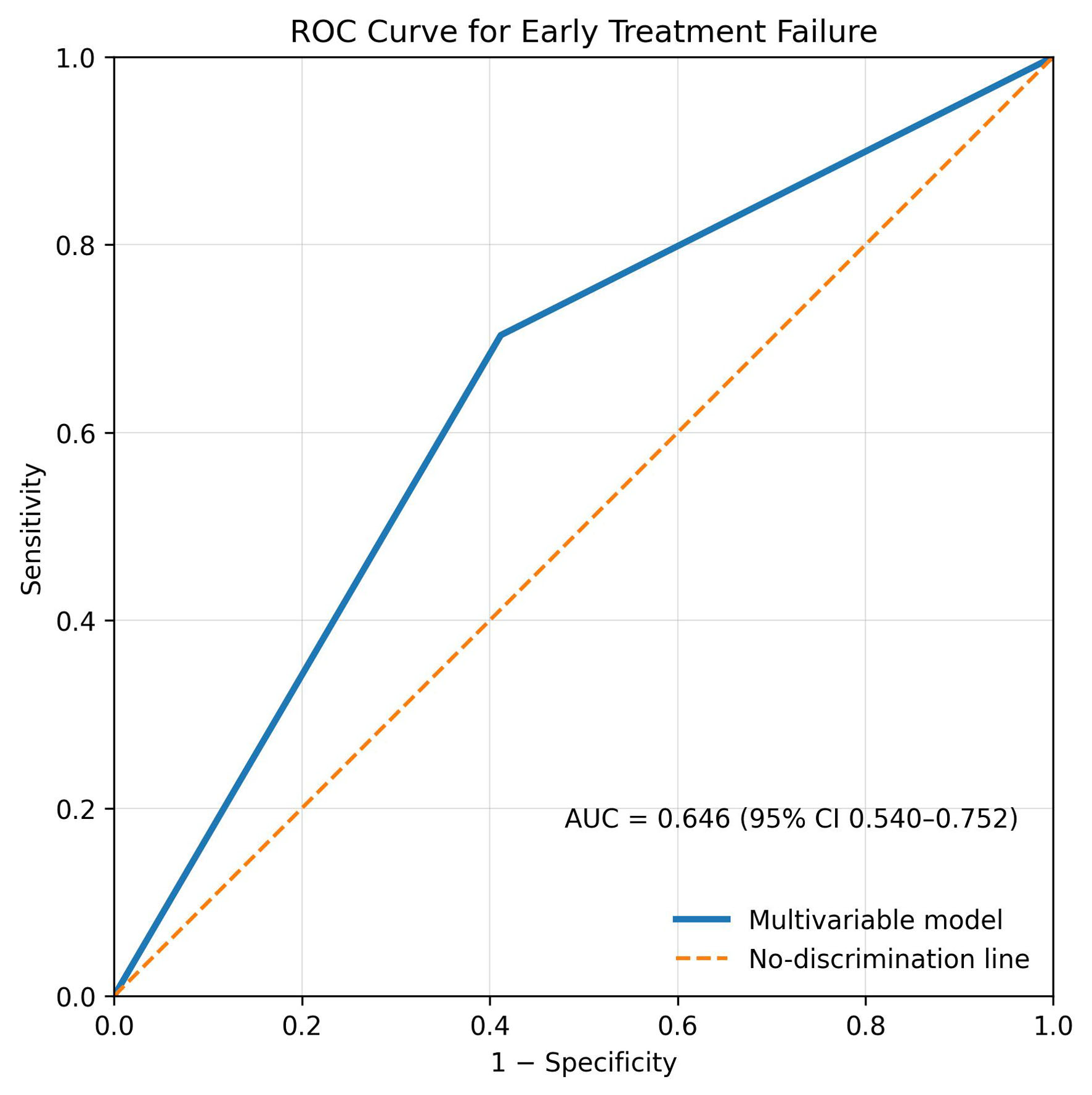
Results: Among 372 patients diagnosed during the predefined study period, 105 with DLBCL were included in the final analytic cohort. Their mean age was 52.2 years and 54.3% were male. Early treatment failure occurred in 54/105 (51.4%): 45 (83.3%) primary refractory and nine (16.7%) early relapse. On univariate analysis, unfavorable ECOG, advanced stage, anemia, and elevated LDH were associated with early failure. In multivariable analysis, only elevated LDH remained independently associated (adjusted odds ratio (OR) 2.41, 95% confidence interval (CI) 1.01–5.79). Model discrimination was limited-to-modest (area under the curve (AUC) 0.646), indicating that baseline clinical variables alone were insufficient for strong individual-level prediction.
Conclusion: In this real-world Indonesian DLBCL cohort, early treatment failure was frequent and was associated with elevated baseline LDH after adjustment. Given the limited-to-modest model discrimination and the retrospective single-center design, LDH should be interpreted as a practical warning marker for closer monitoring rather than a stand-alone predictor, and these findings require prospective validation.
Published
Issue
Section
License
Copyright (c) 2026 The authors

This work is licensed under a Creative Commons Attribution 4.0 International License.





