


Differentiating Juvenile Idiopathic Arthritis From Acute Lymphoblastic Leukemia in Children: A Multidisciplinary Diagnostic Approach, Systematic Review and Meta-Analysis
DOI:
https://doi.org/10.14740/jocmr6630Keywords:
Juvenile idiopathic arthritis, Acute lymphoblastic leukemia, Leukemic arthritis, Differential diagnosis, Thrombocytopenia, Neutropenia, Pediatric rheumatology, Meta-analysisAbstract
Background: Juvenile idiopathic arthritis (JIA) and acute lymphoblastic leukemia (ALL) share overlapping musculoskeletal presentations in pediatric patients, and the misclassification of ALL as JIA carries life-threatening consequences due to inappropriate initiation of corticosteroid or immunosuppressive therapy. A rigorous synthesis of contemporary evidence identifying the most reliable clinical and laboratory discriminators between these two conditions is long overdue. This systematic review and meta-analysis aimed to evaluate clinical, laboratory, and biomarker-based features that differentiate ALL from JIA in pediatric patients. The primary focus was on studies published between January 2021 and April 2026, while selectively incorporating seminal pre-2021 studies with major diagnostic relevance and extractable comparative data to strengthen quantitative synthesis.
Methods: A comprehensive search of PubMed, EMBASE, Web of Science, CINAHL, and Cochrane Library was conducted using pre-specified search terms. Two independent reviewers screened titles, abstracts, and full texts. Methodological quality was assessed with the Newcastle-Ottawa Scale (NOS). Pooled odds ratios (ORs) were estimated under a random-effects model (DerSimonian-Laird), and heterogeneity was quantified using the I2 statistic. Publication bias was evaluated with Egger regression and visual inspection of funnel plots.
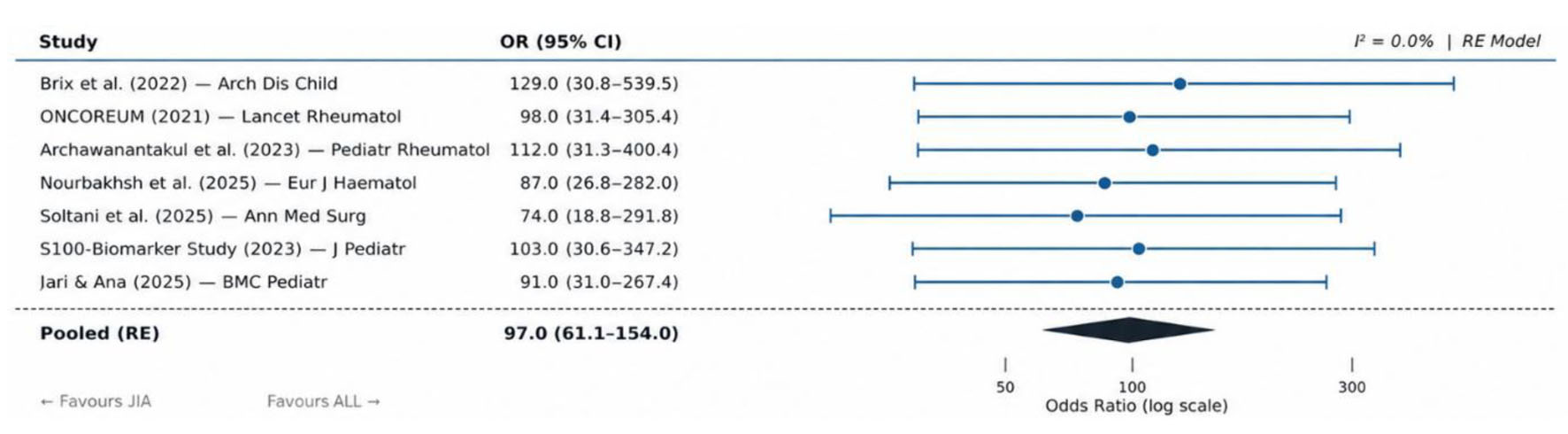
Results: Eighteen studies were included in the qualitative synthesis, of which 12 primary comparative studies contributed quantitative data to the meta-analysis, encompassing 5,198 pediatric patients across 12 countries. Thrombocytopenia (platelets < 100 × 109/L) demonstrated the highest diagnostic weight, with a pooled OR of 108.4 (95% CI: 58.2–201.7; I2 = 34.2%), followed closely by neutropenia (pooled OR = 103.6; 95% confidence interval (CI): 55.9–192.0; I2 = 31.7%) and anemia (pooled OR = 57.4; 95% CI: 22.1–149.0; I2 = 41.6%). Limb pain disproportionate to physical findings, nocturnal bone pain, hepatosplenomegaly, and elevated lactate dehydrogenase (LDH) were additional independent predictors. Novel biomarkers including S100A9 and S100A12 showed markedly reduced levels in ALL compared to JIA (area under the curve (AUC) = 0.91). No evidence of significant publication bias was detected.
Conclusion: The triad of thrombocytopenia, neutropenia, and anemia constitutes the most powerful hematological screening strategy for distinguishing ALL from JIA in children presenting with arthropathy. Bone marrow aspiration should be pursued without hesitation when two or more cell lines are affected. Clinicians must resist initiating immunosuppressive therapy before excluding an underlying malignancy, particularly when pain is nocturnal, disproportionate to findings, or associated with weight loss and organomegaly.
Published
Issue
Section
License
Copyright (c) 2026 The authors

This work is licensed under a Creative Commons Attribution 4.0 International License.





