


Optimizing Rituximab Maintenance Therapy: Outcomes of Extended-Interval Dosing in Multiple Sclerosis and Neuromyelitis Optica Spectrum Disorder
DOI:
https://doi.org/10.14740/jocmr6529Keywords:
Anti-CD20, B-cell depleting therapy, Multiple sclerosis, Neuromyelitis optica spectrum disorder, RituximabAbstract
Background: In many low-resource settings, access to several therapies for multiple sclerosis (MS) and neuromyelitis optica spectrum disorder (NMOSD) is still limited. Although rituximab (RTX) is considered off-label for some indications, it provides a relatively affordable alternative. However, its long-term use raises concerns about adverse effects such as secondary hypogammaglobulinemia and infection. Extending the dosing interval according to circulating cluster of differentiation 19 (CD19) B-cell counts has been proposed to preserve efficacy while minimizing complication and cost.
Methods: This study retrospectively assessed the long-term efficacy and safety of RTX with CD19-guided, extended dosing intervals in patients with MS and aquaporin-4 immunoglobulin G-positive NMOSD. All treatments were delivered at Siriraj Hospital, Thailand, between January 1994 and February 2025. Clinical data, CD19 lymphocyte profiles, immunoglobulin levels and imaging findings were extracted for patients who had received RTX for at least 2 years.
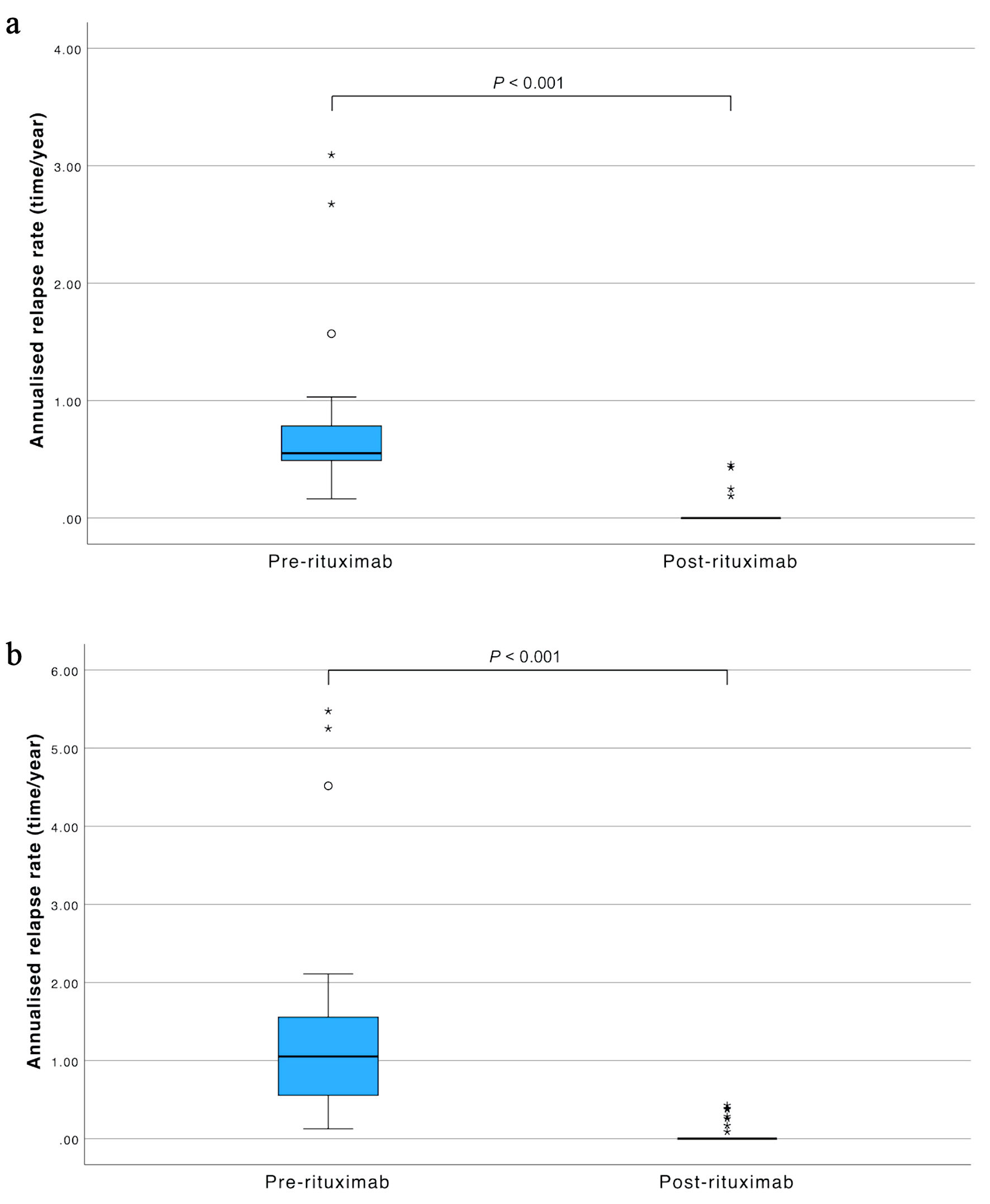
Results: Eighty-seven patients satisfied the inclusion criteria. In the MS cohort of 43 patients, treatment duration (mean ± standard deviation (SD)) was 4.10 ± 1.42 years, and the mean dosing interval was 32.61 ± 4.87 weeks. In 44 NMOSD patients, corresponding values were 4.92 ± 2.32 years and 33.87 ± 8.67 weeks. RTX reduced the median annualized relapse rate from 0.55 to 0.00 in MS and from 1.15 to 0.00 in NMOSD (both P < 0.001). The median Expanded Disability Status Scale scores improved from 2.0 to 0.0 in MS (P = 0.006) and from 4.5 to 4.0 in NMOSD (P < 0.001). Four patients maintained dosing intervals exceeding 48 weeks without relapse, and their CD19-positive B-cell proportion remained below 1%. Adverse events occurred in 32.6% of MS patients and 43.2% of NMOSD patients, most commonly infusion reactions (16.3% and 15.9%, respectively) or infections (14.0% and 27.3%, respectively). Leukopenia was documented in 4.7% of MS and 6.8% of NMOSD patients, whereas hypogammaglobulinemia arose only in NMOSD (6.7%); no fatal events were recorded.
Conclusions: CD19-guided, extended-interval RTX is associated with relapse control, disability score improvement and favorable tolerability, while potentially lowering infusion frequency and healthcare costs in resource-constrained settings. Nonetheless, repopulation of CD19-positive B cells during prolonged intervals warrants vigilance because it may signal an increased risk of relapse.
Published
Issue
Section
License
Copyright (c) 2026 The authors

This work is licensed under a Creative Commons Attribution 4.0 International License.





