


Restrictive Versus Liberal Fluid Strategy for Initial Resuscitation in Sepsis and Septic Shock: A Systematic Review and Meta Analysis
DOI:
https://doi.org/10.14740/jocmr6464Keywords:
Trial sequential analysis, Acute kidney injury, Restrictive fluid, SepsisAbstract
Background: Intravenous fluid resuscitation is essential in early management of sepsis, but the optimal volume and resuscitation strategy are uncertain. This systematic review and meta-analysis aimed to synthesize the evidence comparing the efficacy and safety of restrictive versus liberal fluid resuscitation strategies in adults with sepsis or septic shock.
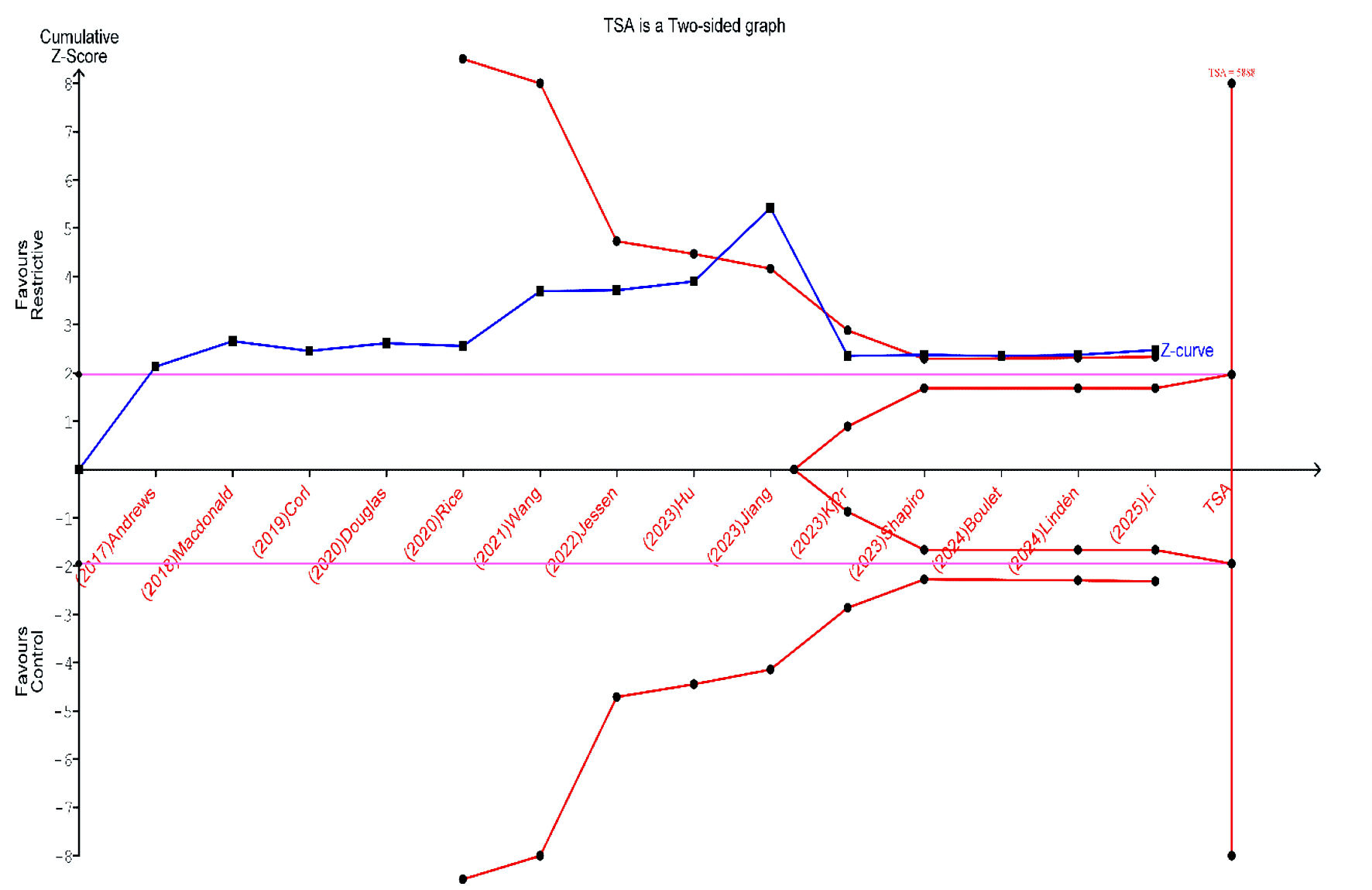
Methods: A systematic search of PubMed, Web of Science (WoS), Scopus, and CENTRAL was conducted from inception to November 2025, following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines. Randomized controlled trials (RCTs) and observational cohort studies comparing protocolized restrictive fluid strategies with liberal or standard care were included. Primary outcomes were all-cause mortality and acute kidney injury (AKI). Random-effects models were used to calculate pooled risk ratios (RRs) and mean differences (MDs), while trial sequential analysis (TSA) assessed the conclusiveness of evidence.
Results: Sixteen reports from 15 unique studies (nine RCTs and six observational studies) involving 5,013 patients were included. In the analysis of RCTs, restrictive fluid therapy resulted in no significant difference in all-cause mortality (RR = 0.99; 95% CI, 0.90–1.08; I2 = 0%); however, observational studies showed a significant mortality reduction (RR = 0.69), suggesting confounding by indication in observational datasets. TSA of the RCT data indicated insufficient evidence for mortality benefit. Restrictive strategies were associated with a lower risk of AKI (RR = 0.89; 95% CI, 0.81–0.99; P = 0.02; I2 = 0%) and a reduced incidence of acute respiratory distress syndrome (ARDS) (RR = 0.69; 95% CI, 0.56–0.85; P < 0.001; I2 = 0%). No significant differences were observed in other ischemic, metabolic, or organ support outcomes. However, restrictive fluid therapy reduced the need for mechanical ventilation, shortened the ventilation duration and vasopressin use, and increased ventilator-free days.
Conclusions: Restrictive fluid resuscitation does not reduce overall mortality in adults with sepsis or septic shock, but it is associated with lower AKI and ARDS risk and decreased dependence on mechanical ventilation. Evidence regarding mortality is inconclusive, highlighting the need for large-scale trials to validate this finding.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 The authors

This work is licensed under a Creative Commons Attribution 4.0 International License.





